New Human Physiology | Paulev-Zubieta 2nd Edition
Chapter 9: Systemic Resistance and Hypertension
| HOME | PREFACE | TABLE OF CONTENTS | SYMBOLS | SECTION INFO | CONTRIBUTORS | LINKS | CONTACT US |
Highlights
Study_ObjectivesPrinciplesDefinitionsEssentials
PathophysiologyEquationsSelf-AssessmentAnswers
Further Reading
|
Chapter 9
|
 |
|
|
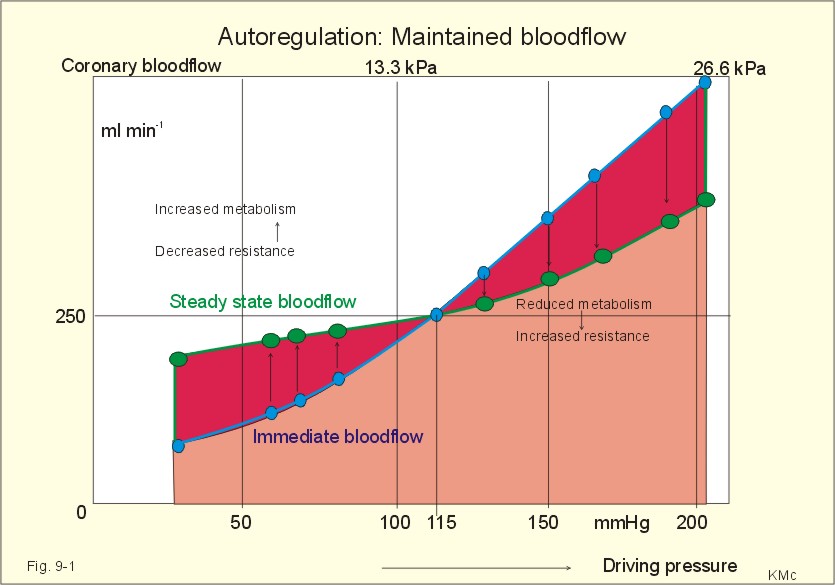
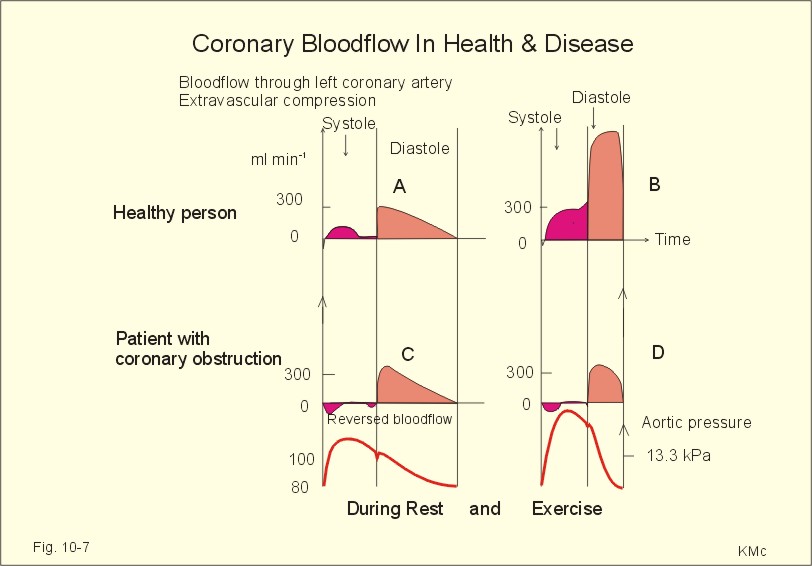
· To define arterioles, autoregulation, mean arterial pressure, metabolic vascular control, preferential channels, systemic hypertension, systemic resistance, and inflammatory hyperaemia. · To describe arteriolar calibre, vascular resistance, the measurement of arterial blood pressure and the pressures of the pulmonary system, the role of myoglobin, respiratory arrhythmia, alterations of mean arterial pressure and pressure amplitude. · To calculate one variable when relevant variables are given. · To explain the control of the arterial pressure, hypertension, and reactive hyperaemia. · To use these concepts in problem solving and in case histories. · The haemodynamic features of the cardiovascular system are determined by Newtonian and non-Newtonian relations between the driving blood pressure, the bloodflow and the vascular resistance. · These features are related to the ability of each tissue to control its own bloodflow in accordance with its needs. The control of local vascular resistance is a combination of neural and metabolic factors affecting a basal smooth muscle tone. · Arterioles are vessels that range from 150 to 10 mm in diameter. They control the distribution of blood to different tissues. · Arteriolar calibre is the internal diameter of the arteriole, and the size is determined by the contractile activity of its smooth muscle cells and by the transmural arteriolar pressure. · Autoregulation is an automatic control phenomenon that aims at maintaining a constant bloodflow when the driving pressure is changed. · Capillary intermittence: Krogh presumed that a tissue capillary shifts between a closed and an open state. The capillary diameter varies with the oxygen tension. In well-perfused tissue, high O2 tension causes vasoconstriction and thus tends to reduce its perfusion. · Inflammatory hyperaemia refers to increased bloodflow with accumulation of leucocytes. This reaction is mainly caused by leukotrienes released by the leucocytes. · Malignant hypertension (accelerated) refers to a rapid and serious rise of the arterial blood pressure. The condition can start as paralysis, unconsciousness, or blindness. · Metabolic control is the sum of all metabolic factors that match the oxygen supply to the energy requirement. · Myoglobin is a red, iron-containing, oxygen-binding globin similar to haemoglobin. · Reactive hyperaemia is the increase in bloodflow following temporal vascular interruption of surgical or experimental character. · Standard affinity of myoglobin towards O2 is the reaction rate at 50% binding. This standard affinity is much higher than that of haemoglobin towards oxygen. · Secondary hyperaldosteronism is recognised by high serum concentrations of renin and aldosterone. This occurs in malignant hypertension or following prolonged use of diuretics. The patients develop cerebral oedema and haemorrhage, cardiac failure and hypertensive nephropathy with proteinuria and microscopic haematuria. · Systemic hypertension - according to WHO - is defined as an arterial blood pressure exceeding 160/95 mmHg (21.3/12.6 kPa) for several months. The pressure increase is either systolic, diastolic or a combination. · Systemic resistance is the total peripheral vascular resistance (TPVR), mainly consisting of the arteriolar resistance (in particular that of the essential arterioles in the large striated muscles). · Thoroughfare channels or preferential channels shunt the blood directly into the venules bypassing the true capillary bed. · Vasomotion is the rhythmic changes in the arteriolar diameter that causes bloodflow to fluctuate. Vasomotion is brought about by active changes in the tension of vascular smooth muscles. The arteriole can relax completely and then close completely. · Vasopressin is another name for anti-diuretic hormone (ADH) from the hypophyseal posterior lobe. ADH controls renal water retention and acts as a moderate vasoconstrictor. · VIP is Vasoactive Intestinal Polypeptide from the intestine, the salivary glands and the penile cavernous bodies. VIP is a neurotransmitter and a potent vasodilatator, which is used in the treatment of impotence. This paragraph deals with 1. Autoregulation, 2. Autonomic nervous control, 3. The baroreceptors and other regulators, 4. Oxygen release to the mitochondria, 5. Measurement of blood pressure, 6. Age and MAP. The resistance vessels of the coronary system tend to diminish any change in the bloodflow in the coronary vessels that are triggered by changes in the driving pressure within a certain range. Increases or reductions in the driving pressure are immediately followed by similar alterations of coronary bloodflow. However, the resistance of the vessels is then changed - metabolically and mechanically - so that the final coronary bloodflow is maintained at control levels at all times (changes along the arrows in Fig. 9-1). Autoregulation has been explained by at least two theories: 1) The myogenic theory considers autoregulation as a myogenic response - an intrinsic property of vascular smooth muscle. Increased stretch of the smooth muscle elicits contraction, whereas diminished stretch elicits vasodilatation. This is illustrated in Fig. 9-1, where an abrupt rise in perfusion pressure from 115 mmHg passively stretches the wall (increases the transmural pressure) and produce an initial increase in bloodflow. Then the vascular smooth muscles contract and the bloodflow falls along the arrows, so that the coronary bloodflow is maintained at 200-250 ml min-1. Similarly, an abrupt fall in perfusion pressure from 115 mmHg has the opposite effect, so the normal bloodflow is re-established. 2) The metabolic control theory.
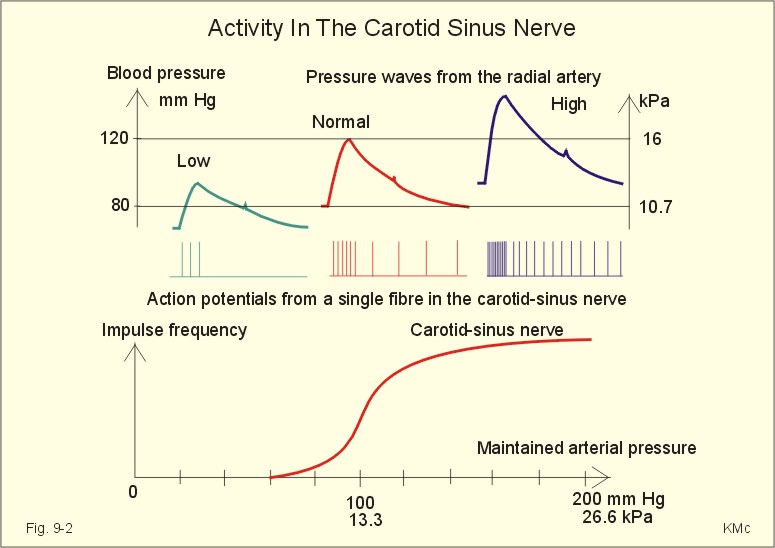
Fig. 9-1: Autoregulation: Changes in bloodflow triggered by changes of the driving pressure has a tendency to be diminished. The example here is the coronary bloodflow, which is described further in relation to Fig. 10-7. Metabolic control is the sum of all metabolic factors that match the oxygen supply to the energy requirement. There is a remarkable proportionality between changes of myocardial oxygen consumption and coronary bloodflow. If the oxygen supply is insufficient compared to the myocardial demand, a vasodilatator is releases from the myocytes to the interstitial fluid, so the coronary resistance vessels dilatate. Adenosine is continuously produced by breakdown of ATP. Adenosine is a likely candidate for the role of metabolic mediator, because it is such a potent vasodilatator and because it diffuses readily across the cell membranes. Adenosine may work via presynaptic inhibition of sympathetic nerve fibres to the smooth muscles of the coronary resistance vessels. Falling perfusion pressure leads to diminished rate of adenosine washout and thus to local vasodilatation. Adenosine dilatates the vessels and causes increased coronary bloodflow. Increased perfusion pressure washes out adenosine, which leads to vasoconstriction and local decrease in bloodflow until it is re-established. - The myogenic and the metabolic control frequently co-operate during autoregulation. Reactive hyperaemia (ie, increased limb bloodflow following experimental vascular interruption) is probably explained by the metabolic vascular control theory. Autoregulation protects not only the coronary bloodflow, but also the cerebral, intestinal and renal bloodflow to mention the most important organs. The sympathetic and the parasympathetic division of the autonomic nervous system control the tone of the resistance vessels by opposing actions. Almost all blood vessels receive efferent nerve fibres from the sympathetic nerve system to their smooth muscles. True capillaries do not contain smooth muscles and do not receive autonomic nerve supply. Metarterioles and capillary sphincters do not receive nerve fibres at all. The sympathetic vasoconstrictor fibres and circulating catecholamines control both arteriolar, venous and venule tone. The vessels are innervated by postganglionic neurons from the paravertebral sympathetic trunk. The noradrenergic control releases noradrenaline and ATP. The transmitter transport is axonal. Noradrenaline binds to a-adrenergic constricting receptors. Adrenaline binds to both a-adrenergic constricting receptors and to b-adrenergic dilatating receptors. Consequently, adrenaline elicits vasoconstriction in arterioles where a-receptors predominate, and vasodilatation where b-adrenergic receptors predominate. Adenosine dilatates vessels, because it inhibits release of noradrenaline possibly via presynaptic purine receptors. In the synapse, the neurotransmitter is eliminated by re-uptake, by enzymatic breakdown and by diffusion. The arterioles of the skeletal muscles, the skin, the kidneys and the splancnic region are densely innervated. Hunting predators are claimed to have sympathetic vasodilatator fibres to the skeletal muscle vessels, which is consequential during hunting, but such fibres have not been found in humans (Uvnaes). The cholinergic system is almost exclusively parasympathetic. The vessels of the head, neck and thoraco-abdominal organs receive parasympathetic nerve fibres (the 3rd, 7th, 9th and 10th cranial nerves). The large intestine, bladder and genital organs receive parasympathetic fibres from the sacral segments 3-5. The nerve fibres to the external genitals are active during sexual excitation. Acetylcholine is the vasodilatating transmitter for muscarinic and nicotinic cholinergic receptors. Purinergic receptors use vasodilatating transmitters as ATP, AMP and the potent adenosine. Cholinergic sympathetic fibres innervate sweat glands and release acetylcholine as stimulus. Rapid regulators of the arterial blood pressure are the arterial baroreceptors originating from the carotid sinuses and the aortic arch. These classical arterial pressor-receptors are well established and work within seconds following dynamic changes in blood pressure. The arterial baroreceptors probably do not regulate chronic blood pressure changes with constant tone. The baroreceptor reflex is triggered by stretch of the wall, and the receptors are also called stretch receptors or pressor-receptors. The baroreceptors are mainly located in the walls of the internal carotid arteries (known as the carotid sinuses) and in the aortic arch. Signals are transferred from each carotid sinus via afferent nerve fibres forming the sinus nerve to the glossopharyngeal nerve, and conducted to the nucleus of the solitary tract of the brain stem. The impulse frequency in the nerve afferents increases with the arterial pressure maintained over a period (Fig. 9-2). The curve is S-shaped with a steep rise in the normal range of arterial pressures, indicating an optimal sensitivity in this area. There is no activity below 60 mmHg. An increasing rate of pressure change (dP/dt; a sudden rise in pulse pressure amplitude) also increases the firing rate in a single nerve fibre (Fig. 9-2, right). Thus, baroreceptors act as differential-sensors. The frequency during the rising systolic pressure is distinctly greater than that in the diastole.
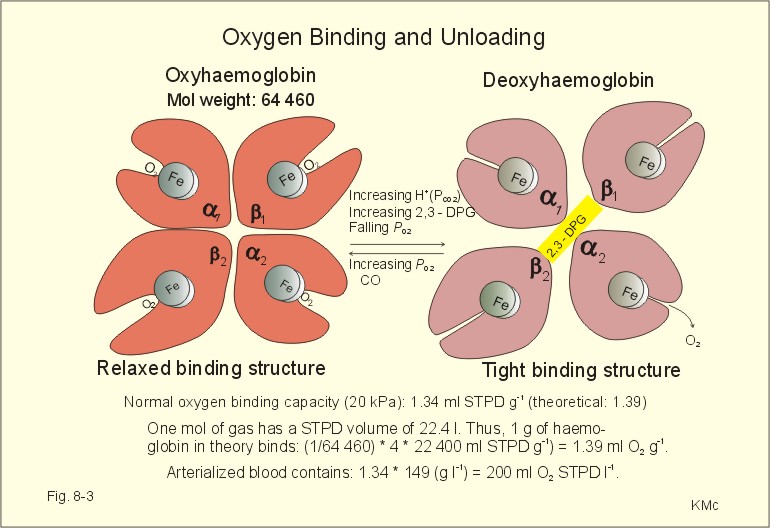
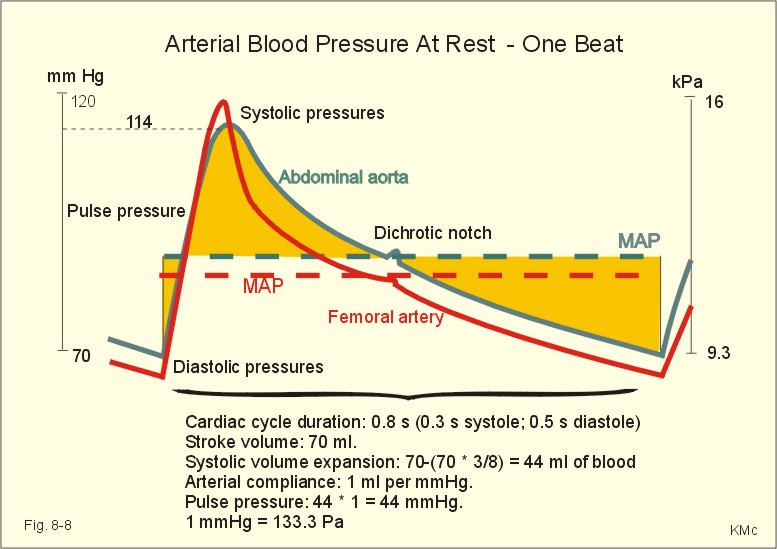
Fig. 9-2: Activity in the carotid sinus nerve at maintained arterial pressure (left) and during a single cardiac cycle with low, normal and high blood pressure. Baroreceptors convey information about mean arterial pressure (MAP), pulse pressure, and the rate of pressure change (dP/dt). Arterial baroreceptor nerve fibres are buffer nerves concerned with short-term buffering of the blood pressure. The afferent signals are conducted to the nucleus of the solitary tract in the medulla. This nucleus is the site confluence for both baroreceptor and chemoreceptor signals. Stimulation here inhibits sympathetic structures and enhances parasympathetic structures. Thus, a rise in arterial pressure causes vasodilatation and a fall in heart rate, both of which contribute to a lowering of blood pressure. A primary fall in arterial pressure elicits vasoconstriction and a rise in heart rate, both of which contribute to a rising blood pressure. Change of body posture from lying to erect reduces the arterial pressure in the carotid sinuses, which elicits an immediate reaction with strong sympathetic tone and diminished vagal tone. This minimises the fall in brain blood pressure, and prevents loss of consciousness. – Hypotensive drugs, exposure to weightlessness, and immobilisation interfere with the baroreceptor reflex, which normally protects us during standing. Such individuals may develop orthostatic hypotension, when they stand up and they may faint. Behavioural and emotional control of blood pressure and heart rate is exhibited by the hypothalamus. This autonomic control centre also includes a temperature centre from where contraction of skin vessels is instituted in cold environments. In hypertension the baroreceptor system adapts to the rising pressure within days by moving up the set point. Patients with hypertension have stiff arterial walls as a result of the high arterial pressure, so their baroreceptors are less sensitive than in healthy persons. The increased arterial stiffness is not the main phenomenon in hypertension. Most hypertensive patients are dominated by increases peripheral vascular resistance, which mainly affects the diastolic arterial pressure. Patients with hypersensitive baroreceptors in the carotid sinuses to external pressures are in danger of hypotension with fainting and death from external pressure over the neck at the site of the carotid sinus (so-called carotid collar syncope or collar death). Tight collars or other types of external pressures elicit fainting due to marked vasodilatation and hypotension. - Another cause is emotional fainting (vasovagal syncope) with a strong emotional activation of the vagus tone via hypothalamus. Three types of regulators are involved in the adjustment of blood pressure. They are classified as short-term, intermediate-term and long-term regulators. 1. The arterial baroreceptor reflexes described above operate rapidly. 2. Transcapillary volume shifts in response to changes in capillary blood pressure, begin their function within minutes. When veins are stressed by increased pressure, they slowly expand so that the blood pressure decreases. Conversely, when the intravascular volume decreases, the opposite occurs. 3. Renal regulation of the body fluid volume. When arterial pressure rises, more urine is excreted. Hereby, the plasma and interstitial volume is reduced. The diminished plasma volume decreases venous return to the heart, reducing cardiac output, so that elevated arterial blood pressure is brought back towards normal (Fig. 9-6). A decrease in arterial pressure elicits the opposite reaction: The renin-angiotensin-aldosterone-cascade is triggered (Chapter 24). Aldosterone from the adrenal cortex promotes Na+-reabsorption and K+-secretion from the renal tubules. The reabsorbed Na+ augments water retention (Fig. 9-6), as does also increased vasopressin (ADH) secretion from the posterior pituitary. A falling arterial pressure also diminishes the release of atrial natriuretic peptide (ANP), and its Na+ - and water- excreting actions are reduced (Fig. 9-6). 4. Oxygen release to the mitochondria The factors that ease O2-diffusion and delivery are: 1. Myoglobin in muscle cells releases O2 during muscular contraction, when the blood supply is blocked. Myoglobin is important as a dynamic O2 store in muscle cells, although myoglobin is not totally saturated with O2. During muscular contraction the bloodflow is blocked, and the O2 tissue tension falls drastically. Myoglobin then gives off O2 to the cell. The P50 for oxymyoglobin is only 5 mmHg (compare to 27 mmHg for oxyhaemoglobin). Bloodflow is re-established during muscular relaxation. Thus, myoglobin is rapidly reloaded, even when there is only a small rise in O2 tension. 2. Heat energy releases O2 during work, since increasing heat energy equals increasing movement of O2 molecules. 3. Carbon dioxide: With rising PCO2, oxygen binding to haemoglobin decreases (Bohr effect, Fig. 8-3). 4. Binding of 2,3 - DPG (diphosphoglycerate) to haemoglobin eases the release of O2 at low tensions (see Chapter 8, paragraph 3). 5. Mitochondria located close to capillaries have reduced diffusion pathway. 6. Short distance capillary networks, as following capillary recruitment, improve the oxygen delivery. Oxygen is lipophilic. Since almost the entire capillary surface is identical to the lipid containing plasma membrane of the endothelial cells, oxygen is able to use the total capillary surface for diffusion. The transport of lipophilic molecules is perfusion limited. Oxygen diffuses so easily over the capillary endothelium, that there is tension equilibrium between blood and tissues already at the arterial capillary end. With rising perfusion the tension equilibrium point is shifted towards the venous part. Due to the oxyhaemoglobin, the O2 tension can be maintained through the entire capillary. The oxygen tension varies in the tissues. There is a longitudinal tension drop towards the venous end of the capillary, and radial tensions drop in the tissue itself. In brain tissue, the O2 tension can vary from an arterial level in certain small areas (PaO2 of 13.3 kPa or 100 mmHg) towards zero, when bloodflow is insufficient. Brain and heart tissues are extremely sensitive to a fall in PO2. Brain tissue is found in the nerve cells of the retina. These nerve cells are deprived of oxygen in 4.5 s (occurrence of black out). This can be verified by pressure on the upper eyelid. Consciousness is lost (grey out) a few seconds after cardiac arrest. After 90 s, the brain interstitial fluid [K+] increases drastically from 3 to 60-70 mM, and both action potentials and synapse transmissions are eliminated. There is ion equilibrium over the cell membranes. Intracellular [Na+] also increases drastically and intracellular brain oedema develops. A high extracellular [K+] is life threatening. The EEG of an anoxic brain is recognisable as a straight EEG trace (no electrical activity) indicating brain death. Because [Ca2+] rises in the nerve cell, this increases the K+ conductance, so that more K+ leaks out into the interstitial fluid. The kidneys only use 15 ml O2 each min but they receive 25% of the cardiac output at rest (1200 ml per min containing 200 ml O2 per l). The kidneys have the lowest arteriovenous O2 content difference of all the larger organs in our body. The large safety margin is important for this vital organ during bleeding or when the renal bloodflow is reduced (more in Chapter 25). 5. Measurement of blood pressure The arterial blood pressure is measured indirectly in the brachial artery with Korotkoff´s auscultatory method. WHO has proposed standardisation of this method. Continuous intra-arterial recordings can obtain exact arterial blood pressure measurements. Comparison with intra-arterial recordings have shown that Korotkoff´s method estimates the systolic pressure too low (about 10 mmHg), and the diastolic pressure differs a few mmHg. The blood pressure increases in some patients due to the presence of a doctor (ie, white coat hypertension). This is revealed by repeated measurements – preferably performed before, during and following exercise. Ejection of blood from the left ventricle triggers a pulse wave in the wall of the arterial tree, and the volume-pressure variations here distribute with a large velocity along the arterial tree. In young persons the velocity is 5-10 m per s; with age, atherosclerosis and hypertension the arterial tree becomes stiffer and the velocity increases (see Ch. 8 about compliance and also Fig. 8-8).
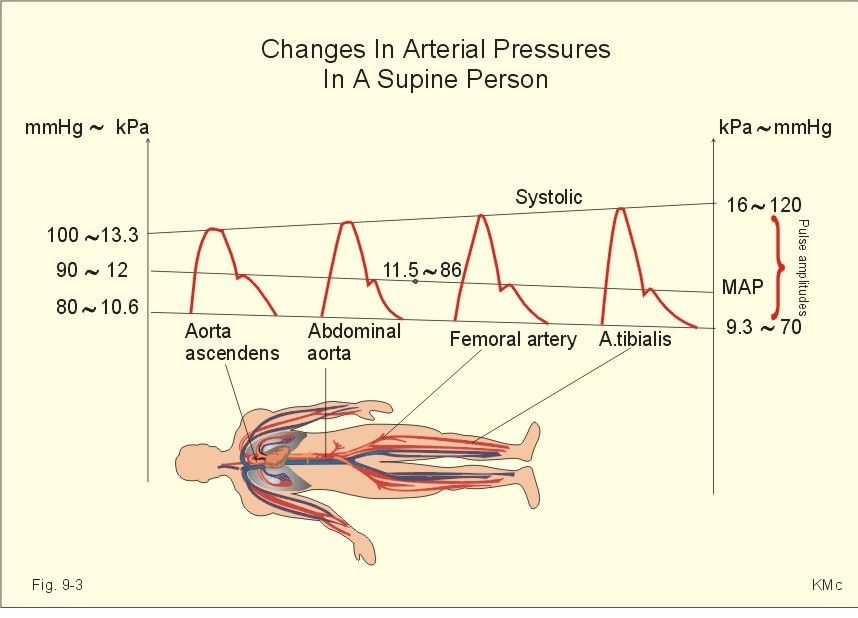
Fig. 9-3: Changes in pressure in the arterial tree of a supine healthy person. The systolic pressure increases progressively along the arterial tree, whereas the diastolic and the MAP decrease (Fig. 9-3). The pulse amplitude, which is the difference between systolic and diastolic pressure therefore, increases clearly (Fig. 9-3). The end of systole is marked by a brief sharp fall in pressure (dicrotic notch), caused by the relaxation of the ventricle with backflow of blood as the aortic valves close. This backflow pressure moves with the blood all along the arterial tree (Fig. 9-3). The blood pressure has to be measured repeatedly, with the patient sitting comfortably in a relaxed environment, and measured at more than three consultations in order to avoid false alarm with white coat hypertension. A diastolic pressure above 95 mmHg (12.6 kPa) expresses an increased MAP and the age of the patient influences the strategy of the treatment.
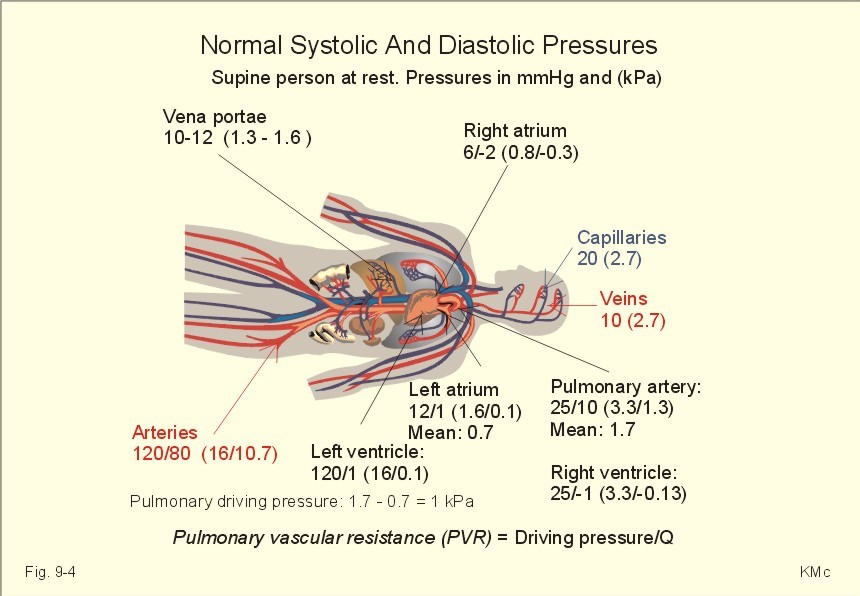
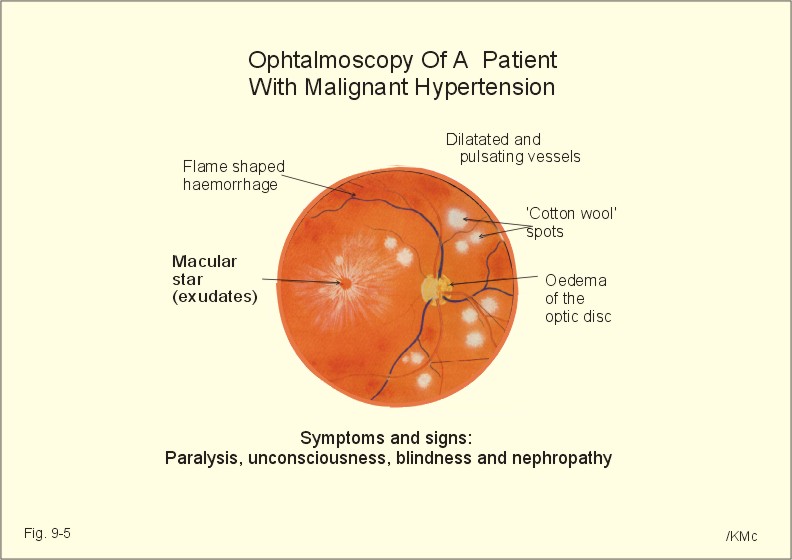
Fig. 9-4: Normal pressures in the circulation of a supine healthy person. Essential diurnal variations are present, but repeated blood pressure measurements over three consultations seem to define a reasonable diurnal mean level. Continuous recording of the arterial pressure is sometimes necessary. Patients below 40 years of age, with a diastolic pressure above 100 mmHg must be followed and examined further. Patients above 40 years of age, with a diastolic pressure above 120 mmHg, must be examined further. Normal values for blood pressures measured in different locations of the circulation are given in Fig. 9-4. Populations living under natural conditions - including Indian troops in Brazil and healthy living persons in the Western Hemisphere - maintain their mean arterial pressure (MAP) throughout life. Their distribution curve for MAP is close to the normal distribution. The MAP and the systolic pressure measured as an average for the total population, increases with increasing age in the rich part of the World. As an order of thumb, the systolic blood pressure in mmHg is equal to 100 plus age in years, because these values are close to typical statistical mean values from examination of large population groups. This is because general diseases, with consequences for the systolic blood pressure and MAP, are accumulated with age in the Western Hemisphere. Quite a few of the accumulated disorders (such as atherosclerosis – see Chapter 10) probably occur as a consequence of our life style - operating in a heterogeneous genetic pool. Previously, systemic hypertension was therefore characterised by a MAP larger than normal for the age. Practically difficult comparisons had to be made with a statistical, so-called normal material. Today, most doctors use the WHO definition (see below). The MAP is a good estimate of the driving pressure, and the cardiac output is the stroke volume multiplied by the cardiac frequency. MAP and cardiac output are easy to determine, so the TPVR can be calculated. With pressure expressed in mmHg and cardiac output expressed in ml per s, the unit for TPVR is 1 mmHg*s*ml-1. This unit is complicated in writing and the abbreviation is 1 PRU (Pressure Resistance Unit). The normal value for TPVR in the systemic circulation at rest is one PRU, and during exercise it is only 0.3 PRU. Pathophysiology This paragraph deals with 1. Natural history of hypertension, 2. Symptoms and signs of hypertension, 3. Risk factors (Western lifestyle), 4. Types of systemic hypertension, 5. Therapeutic principles, 6. Future strategy. 1. Natural history of hypertension Primary hypertension always has a diastolic element reflecting involvement of the resistance vessels (eg, muscular arterioles etc). Secondary hypertension, caused by atherosclerosis or other types of stiff arterial walls, is often purely systolic. In the early stages of hypertension, the arterial blood pressure is oscillating between hypertensive episodes and normal periods. The hypertensive episodes are typically dominated by sympathetic overactivity with increased cardiac output and almost unchanged total peripheral vascular resistance (TPVR). Eventually, the pressure changes the distensibility of the arteriolar walls and thus leads to sustain structural changes of the resistance system. As the hypertension develops the TPVR is increased. Any rise in blood pressure is a strong stimulus to the high-pressure baroreceptors, but these essential sensors do not always work appropriate in hypertension. The expected bradycardia from the high arterial pressure acting normally on the arterial baroreceptors is not seen in hypertensive patients. The initial sympathetic tone is also depicted in the high resting heart rate, in contrast to the bradycardia found normally, when the blood pressure rises. The abnormal baroreceptor reflex is probably an adaptive consequence of the variable but lasting initial hypertension. Permanent structural changes of the resistance vessels, with strongly reduced specific compliance (reduced distensibility) and reduced lumen of arterioles and small muscular arteries, eventually leads to permanent hypertension. The rising TPVR implies a rising workload for the left ventricle and thus creates left ventricular hypertrophy. 2. Symptoms and signs of hypertension The typical patient with hypertension is asymptomatic. This is what makes the development of this disorder dangerous. The first sign of systemic hypertension is sometimes acute myocardial infarction with sudden death. Of all acute cases of myocardial infarction up to 25% only experience a sudden pain, there is cardiac arrest, and the cases are recorded as sudden death from myocardial infarction at section. Hypertonic patients with coronary artery disease experience angina at exhaustion or from myocardial hypertrophy. Malignant or accelerated hypertension refers to a rapid and serious rise of the arterial blood pressure. The condition can start as paralysis, unconsciousness, or blindness. Secondary hyperaldosteronism is recognised by high serum concentrations of renin and aldosterone. This occurs in malignant hypertension or following prolonged use of diuretics. The patients develop cerebral oedema and haemorrhage, cardiac failure and hypertensive nephropathy (with proteinuria and microscopic haematuria). Patients with malignant hypertension develop dissecting aortic aneurysms and retinal damage with papiloedema, so they die rapidly without specific therapy. Ophtalmoscopy for hypertonic changes of the retina also provides the diagnosis hypertension. These changes include haemorrhages in the retinal nerve fibre layer, exudates as yellow-white spots called cotton wool spots, irregular arteriolar diameter, microaneurysms, and papillary stasis (Fig. 9-5).
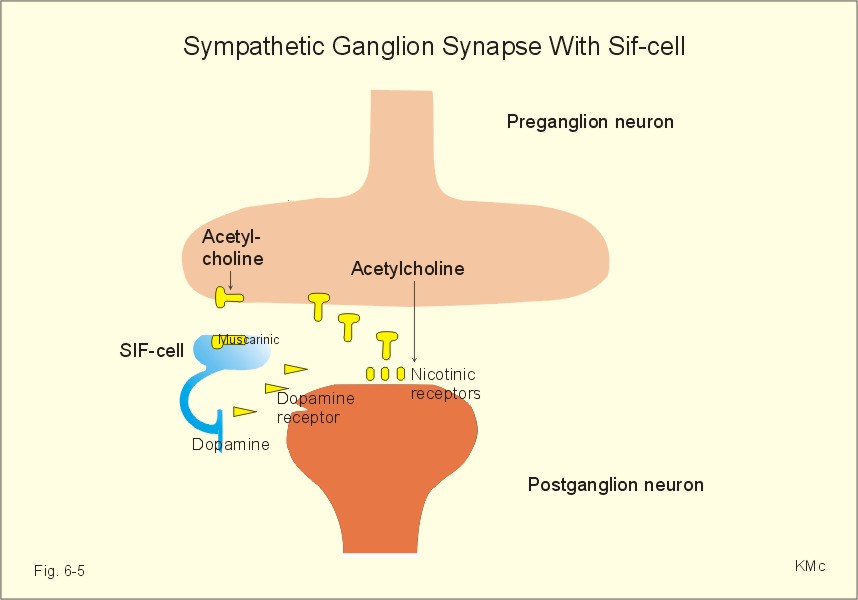
Fig. 9-5: Hypertonic changes of the retina seen by ophtalmoscopy. The patient has malignant hypertension. - A normal retinal fundus is found in Fig. 6-5. A necrotic arteriolitis is often found by ophtalmoscopy in malignant hypertension. 3. Risk factors (Western lifestyle) Causative or risk factors for essential hypertension include genes, because there is a clear racial and familial accumulation of hypertension. A risk factor is a factor showing statistical covariance with the disease - see also Chapter 10. Africans have higher arterial blood pressure than Caucasians, and some families accumulate cases of hypertension. Specific genes have not been identified. The environmental factors are numerous, but Western Hemispher lifestyle is the key word, since the occurrence of increasing systemic blood pressure with increasing age is obviously related to accumulation of disease. However, accumulation of hypertension with age is not a law of nature. Western lifestyle is sedentary, with psychological stress in career and family life. Existential procedures have to be performed rapidly including buying and eating fast food. Persons with a stressful everyday life, with smoking, alcohol and large meals following long work hours, practice little exercise if any, and become obese with hyperlipidaemia, hyperglycaemia and hyperuricaemia. The hunting human has become a stressed user of automatic tools (cars, mobile telephones, household utilities, TV, PC etc). This lifestyle pattern frequently implies a serious sympathetic overactivity with a typical rise in resting cardiac rate and thus in cardiac output. One essential and measurable variable in the life style pattern is the lack of exercise (eg, physical inactivity). A low maximum oxygen capacity or fitness number is measurable with the submaximal exercise test of Åstrand (Fig. 18-3), and reproducible in each individual. The fitness number is expressed as the maximum oxygen uptake in ml*min-1*kg-1. A maximum oxygen uptake below 34 (ml*min-1*kg-1) is related to risk factor accumulation and early death from hypertensive or other related complications (Fig. 18-14). Such a low maximum uptake is a clear indication of physical inactivity, where dilatation of muscular arterioles is seldom or almost never achieved. The unknown cause of essential hypertension in the Western Hemisphere may well prove to be physical inactivity and the related life style patterns described above. In some cases of hypertension there is a clear relation to the renin-angiotensin-aldosterone cascade (Chapter 24). The series of events starts with a rise in TPVR due to increased vascular tone. Over months and years, the walls of arteries and arterioles thicken and atherosclerosis is spread in the arterial tree. Such changes reduce the driving pressure in the renal arteries, which leads to a fall in glomerular filtration rate (GFR) and increased NaCl/water retention (Chapter 25). The falling pressure in the renal artery triggers b-receptors on the JG-cells of the juxtaglomerular apparatus (Fig. 25-17). Renin is released from these cells located in the afferent glomerular arteriole. Renin separates the decapeptide, angiotensin I, from the liver globulin, angiotensinogen. When angiotensin I passes the lungs or the kidneys, a dipeptide is cut off from the decapeptide by an angiotensin-converting enzyme (ACE). Hereby angiotensin II (octapeptide) is produced. Angiotensin II stimulates the aldosterone secretion from the adrenal cortex, and thus stimulates the Na+ reabsorption and the K+ secretion in the distal, renal tubules. The renin-angiotensin-aldosterone cascade further contributes to the salt and water retention. Angiotensin II is also a circulating vasoconstrictor just as adrenaline and vasopressin found in high plasma concentrations in many hypertonics. ACE inhibitors (see later) are rational choices for hypertonics with high angiotensin II, but also for other categories for reasons unknown (diabetics etc). The cascade is further described in Chapter 24 – paragraph 6. 4. Types of Systemic Hypertension There are two forms of hypertension, I) primary or essential, and II) secondary hypertension. I) Primary hypertension is a multifactorial syndrome without known cause. Approximately 90% of all cases are classified as primary or essential hypertension, because the causative factors are not clarified in detail. Increased peripheral resistance is responsible for most cases of primary hypertension.
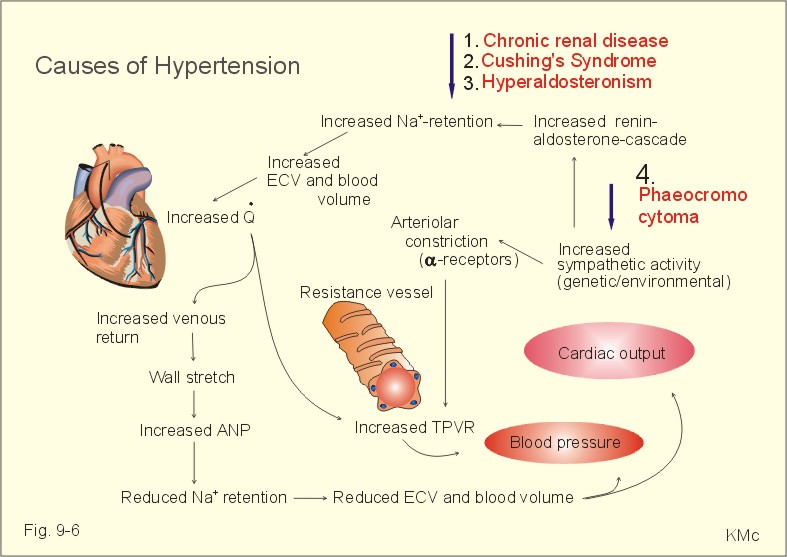
Fig. 9-6: Factors contributing to systemic hypertension. Abbreviations: ECV = Extracellular fluid Volume; TPVR = Total Peripheral Vascular Resistance. II) Secondary hypertension In about 10% of all cases the cause of the hypertension is clarified, and these patients are classified as secondary hypertension. This condition must always be suspected in young hypertonics. Renal, endocrine or cardiovascular diseases cause secondary hypertension or it relates to pregnancy or to drugs. Endocrine disorders are treated systematically in Chapters 26-30. 1. Renal disorders (Chapter 25) account for more than 80% of all cases of secondary hypertension. The disorders are chronic cases of glomerulonephritis, pyelonephritis and other permanent damage of the kidneys, where salt and water retention dominates. Hyperparathyroidism and Ca2+ overload can lead to renal failure and severe hypertension. A renal artery stenosis sufficient to reduce the glomerular pressure leads to renin release from the juxtaglomerular apparatus, aldosterone release and thus to increased salt-water retention (see the renin-angiotensin-aldosterone cascade, Chapter 24, paragraph 6). Renal artery stenosis (atherosclerosis or fibromuscular hyperplasia), chronic renal inflammation (glomerulonephritis or pyelonephritis), and congenital polycystic kidneys can lead to secondary, systemic hypertension. Renal function is examined with endogenous creatinine clearance and the renal vessels by scanning or arteriography. The plasma renin concentration is measured. - Dopamine D3 receptors seem to be deficient in the development of salt-dependent hypertension (Luipold et al., 2001). 2. Hyperaldosteronism has a primary and a secondary form. Conn´s syndrome is primary hyperaldosteronism. This condition is characterised by an isolated rise in serum aldosterone, since the cause is hyperfunction of the zona glomerulosa of the adrenal cortex - not the renin release. Secondary hyperaldosteronism is a condition with abnormally high stimulation of the adrenal zona glomerulosa. The serum concentrations of the whole renin-angiotensin-aldosterone cascade are increased. 3. Cushing’s syndrome describes clinical conditions with increased glucocorticoid concentration in the blood plasma. The classical Cushings disease is caused by excess liberation of ACTH from the adenohypophysis, but ACTH excess is also known to originate from ectopic ACTH producing tumours or from excess administration of ACTH. - Non-ACTH related adrenal adenomas or carcinomas, glucocorticoid excess administration, and alcohol abuse (so-called Pseudo-Cushing) cause Cushing’s syndrome. - The dexamethasone suppression test is described in Chapter 30. 4. A pituitary tumour producing an excess of growth hormone (Ch.28) causes acromegaly. The patient sometimes has a diabetic glucose tolerance test (Ch.27). These patients die from heart failure, IHD or hypertension. 5. Phaeochromocytoma. This is a tumour of the sympathetic nervous system (Ch. 28) releasing both noradrenaline and adrenaline. The signs are intermittent or constant systemic hypertension, tachycardia with other arrhythmias, orthostatic hypertension and flushing. 6. In the last three months of pregnancy some females develop hypertension, oedema and proteinuria (pre-eclampsia or toxaemia of pregnancy). If this condition develops into severe hypertension with fits and lung oedema, it is called eclampsia. This is a life threatening condition, which must be treated immediately with intravenous hydralazine or minoxidil, and if necessary termination of pregnancy. Hydralazine is orally active vasodilatators, which work by direct relaxation of smooth muscles. 7. Drugs such as steroids or oral contraceptives with high oestrogen, sympatomimetics, aldosterone, and vasopressin all cause severe systemic hypertension. Monoamineoxidase-inhibitors combined with tyramine (cheese) or wine sometimes cause hypertension. A careful medical history is helpful. 8. Cardiovascular disorder - as coarctation of the aorta - is the cause of hypertension in a few young patients. The coarctation produces a late systolic murmur. These hypertonics have a low pressure distal to the coarctation. 9. Atherosclerosis (see Chapter 10) is characterised by a special systolic hypertension frequently found in the elderly without any diastolic hypertension. These patients do not have any arteriolar disease. Systemic hypertension is a health threat to the person as a whole, since the untreated disease shortens life expectancy with approximately 20 years. Target organs for damage are the heart, aorta, brain, eyes and the kidneys. The positive effect on life expectancy of a moderate reduction of an abnormally high systemic arterial blood pressure is well documented. The simple resistance model presented in Eq. 9-1 is applied for the therapy of systemic hypertension. The driving pressure in the systemic circulation is equal to the cardiac output multiplied with the Total Peripheral Vascular Resistance (TPVR). The cardiac output is equal to the cardiac frequency multiplied with the stroke volume, and the stroke volume depends of the total blood volume. TPVR depends of the degree of contraction of the resistance vessels and of the distensibility (eg, specific compliance) of the arterial system. Principally, systemic hypertension is therefore treatable through one or more of the following strategies: 1. Reduction of the total blood volume (and thus the stroke volume) with diuretics results in reduction of the driving pressure, 2. Reduction of the cardiac frequency reduces cardiac output and thus the driving pressure, 3. Reduction of TPVR with vasodilatators reduces the driving pressure. Two strategies of therapy and their combination are available: Change of life style with or without drug therapy. Drug therapy must usually be continued for the lifetime of the patient. Life style modifications (relaxed duration exercise and healthy habits): In healthy individuals, the opening of resistance vessels during exercise typically reduces the TPVR to 30% of the value at rest. This vasodilatation expresses an enormous capacity, which is only present in the resistance vessels of the striated muscular system at large. The only natural way to break the vicious circle described above is to maintain the dilatation capacity throughout life by frequent use of the locomotor system. The exercise must include large muscle groups for some time. The exercise must be relaxed and comfortable in order to become a life style. Other beneficial effects of relaxed duration exercise (such as walking, golf, jogging, swimming, badminton, tennis etc) is improved glucose tolerance, weight loss, improved heart function, improved lipid profile, normal gastrointestinal functions and psychological benefits such as improved mood and a healthy sleep pattern. Healthy food and drinking habits are important, and smoking has to be given up. Hypotensive drugs can be divided into 5 categories: Hypertensive patients seem to handle Na+ just as healthy persons (see Chapter 25). Initial administration of diuretics produce a pronounced renal salt and water excretion, which lead to a reduction in ECV, and a fall in systemic blood pressure. The urinary salt and water excretion returns to normal after several days, but the blood pressure remains at the reduced level. This is difficult to explain. Perhaps some diuretics have a direct relaxing effect on vascular smooth muscle in the arterioles or other vessels. The different groups of diuretics are treated in Chapter 25. 5.2. b-adrenergic receptor blockers b-blockers antagonise competitively the effects of adrenaline and nor-adrenaline on b-adrenergic vasodilatating receptors. The typical non-selective b-adrenergic receptor blocker is propranolol, which is a potent reversible antagonist at both b1-and b2-adrenergic receptors. Propranolol acts on the heart and reduces the chronotropic (reduced heart rate) and inotropic effect (reduced force and cardiac output); the reduced cardiac function is most pronounced during high sympatho-adrenergic activity, such as during exercise or stress, so the drug can release acute cardiac failure. The anti-arrhythmic effect of propranolol is probably due to its local anaesthetic action on cardiac cells including pacemaker cells. The effect of propranolol on hypertension is not clarified, since it seems to increase peripheral vascular resistance slightly. Simultaneously, propranolol reduces the release of renin from the juxtamedullary apparatus. This inhibits aldosterone secretion, and thus reduces the potassium secretion of the distal tubular system. The result is potassium retention, which is further aggravated by b-blockade of receptors on cell membranes, whereby the adrenaline-stimulated Na+-K+ pump is inhibited. Following meals containing carbohydrate and potassium, there is a release of insulin, which stimulates the Na+ - K+ pump, and thus the K+ uptake in cells. Adrenaline also stimulates the Na+- K+pump through activation of b2 - receptors, whereby the plasma-[K+ ] is reduced. The normal effect of insulin is hypoglycaemia, which is compensated by lipolysis and glycogenolysis (with FFA and glucose liberation), by increased sympathoadrenergic activity. Propranolol inhibits lipolysis from adipocytes and glycogenolysis from hepatocytes, myocardial and skeletal muscle cells. This is a problem with diabetics or for patients with reduced glucose tolerance. b-blockade may lead to life threatening hypoglycaemia or a serious rise in blood pressure, if adrenaline release dominates. Propranolol is thus contraindicated in persons with diabetes, sinus bradycardia, partial heart block and congestive heart failure. Propranolol increases airway resistance, which is a hazard to patients with COLD or asthma, because of bronchoconstriction. Many b-blockers act selectively, but all compounds have effects as described below: Selective b1-blockers acts on the cardiac b1-receptors and reduces the force of cardiac contraction and thus lowers the blood pressure. Blockade of b1-adrenergic receptors located on the renin-secreting juxtaglomerular cells reduces the renin release and the blood pressure in persons with renin-dependent hypertension (eg, patients with a high renin level in the plasma from renovascular disease). Many b-blockers reach the brain tissue through the blood-brain barrier, and others reach the brain cells through the large fenestrae of the circumventricular organs. The CNS-effect is an inhibition of the sympatho-adrenergic output, and beneficial effects on paroxysms of panic and anxiety. The hypotonic CNS-effect is probably dominating, and explains the maintained lowering of blood pressure, although the initial reduction in cardiac output is often only temporary. 5.3. a1-adrenergic antagonists inhibit the effect mediated through noradrenaline released from sympathetic presynaptic fibres to the postsynaptic a1-receptors and produce vasodilatation. Also a central effect of these compounds (doxazosin, prazosin) may be involved. The hypotensive efficiency of these drugs give rise to the main complication, which is a serious fall in blood pressure following the first dose. 5.4. Angiotensin Converting Enzyme (ACE) Inhibitors Angiotensin converting enzyme is found to have the highest activity in the endothelium of the long pulmonary capillaries. Converting enzyme is a kininase II, which convert the decapeptide, angiotensin I, to the vasoconstrictive octapeptide, angiotensin II. ACE inhibitors (captopril, enalapril, and lisinopril) reversibly inhibit converting enzyme and thus act as a vasodilatator of both resistance and capacitance vessels. Angiotensin II is a potent vasoconstrictor, in particular when its concentration in plasma is high. Patients with 100 pg l-1 or more of angiotensin II react beneficial on ACE inhibitors. Also other hypertonics such as diabetic patients reduce their risk of vascular insults by the use of ACE inhibitors for reasons unknown. 5.5. Calcium-channel blocking agents Ca2+-antagonists (amlodipine, nifedipine, diltiazem, and verapamil) acts as effective vasodilatators, because they relax the smooth muscles of the arterioles. They also inhibit the cardiac contractile force. Ca2+ -antagonists inhibits the Ca2+ -entry into the cells, because they bind to the proteins of Ca2+ -channels in the membrane. The overall effect is beneficial incongestive heart failure, because the vasodilation dimishes TPVR and thus reduces afterload. Hereby, the cardiac output is improved despite cardiac contractile depression. · Systemic hypertension is the most frequently diagnosed and treated risk factor for the development of atherosclerosis (including ischaemic heart disease). · A risk factor is a factor showing covariance with atherosclerosis. The remaining risk factors for atherosclerosis are physical inactivity, hypercholesterolaemia, hypertriglyceridaemia, increased LDL concentration, smoking, diabetes, and familiar factors (genes, social inheritance or life style patterns). · A rational strategy is to control the risk factors for the patients. A successful lowering of arterial blood pressure with a hypotensive drug must not be accompanied by an unrecognised consequential rise in other risk factors. · Relaxed exercise is an alternative therapeutic strategy to antihypertensive drugs in many cases of essential hypertension. · Mild and relaxed exercise has other beneficial effects, namely a consequential reduction of most of the known risk factors for atherosclerosis. · Healthy food, exercise and drinking habits are important to hypertonics, and smoking has to be given up. The driving pressure (DP) in the systemic circulation is equal to the cardiac output (Q °) multiplied with the TPVR according to Poiseuille´s law: Eq. 9-1: DP = Q° * TPVR. This is a simple resistance model for circulating fluid, and the model is applied for therapeutic strategies. Fick's first law of diffusion: The flux (J) of O2 is equal to the diffusion coefficient of oxygen (D is 10-9 m2 s-1) multiplied with the concentration gradient (dC) per distance unit (dx) through a given area (A). Fick's first law is written: Eq. 9-2: J = ( - D × dC)×A/dx (mol per time unit) with a diffusion gradient (dC) through the area A. Notice that D/dx is a permeability coefficient (m per s). The first law can also be written: J = (D × DP × A)/dx. I. The following five statements have True/False options: A. Nitrovasodilatators has side effects such as hypotension, reflex tachycardia and headache. B. The blood-brain barrier is impermeable to all b-blockers. C. The ACE-inhibitor, captopril, dilatates both arterioles and capacitance vessels. D. Depolarisation of the vascular smooth muscle cell membrane opens voltage-gated Ca2+ -channels, whereby Ca2+-ions enter the cell, combine with calmodulin and activate myosin light-chain kinase. E. Thiazides have serious side effects such as hyperglycaemia (glucose intolerance), hypercholesterolaemia, hypokalaemia and hyperuricaemia. II. The following five statements have True/False options: A. MAP and Q° are easy to determine, so the TPVR can be calculated. B. Angiotensin converting enzyme is a kininase II, which convert the decapeptide, angiotensin II, to the vasoconstrictive octapeptide, angiotensin I. C. The driving pressure (DP) in the systemic circulation is equal to the cardiac output (Q° ) divided by the TPVR according to Poiseuille´s law. D. Noradrenaline binds to a-adrenergic constricting receptors. Adrenaline binds to both a-adrenergic constricting receptors and to b-adrenergic dilatating receptors. Consequently, adrenaline elicits vasoconstriction in arterioles where a-receptors predominate and vasodilatation where b-adrenergic receptors predominate. E. Ca2+-antagonists (amlodipine, nifedipine, diltiazem, and verapamil) act as effective vasodilatators, because they relax the smooth muscles of the arterioles. A male, age 50 years, visits an ophthalmologist in order to have measured new lenses for myopia and astigmatism. Ophtalmoscopy reveals irregular vessel diameter, bleeding, yellow-white spots, and papillary stasis. The patient is advised to see his general practitioner, which finds a constant arterial blood pressure of 200/110 mmHg (26.66/14.66 kPa). The heart frequency is 85 beats per min and the cardiac output at rest is normal. The patient is an office clerk, and also has a sedentary off- duty life. The patient is a heavy smoker using 40 cigarettes per day. His father had high blood pressure and died from cerebral infarction at the age of 62 years. An X-ray of thorax reveals clear lung fields and left ventricular hypertrophy. 1. What is the diagnosis? 2. What is the treatment of choice? 3. What is the main risk for this patient? 4. What happens in the lungs and the left ventricle of this patient? 5. Compare the left ventricular pressure-volume work rate of this patient to that of a healthy individual. Assume that they are both at rest with a cardiac output of 5 l per min. Assume that the healthy person has a mean arterial pressure of 90 mmHg (12 kPa). 6. Convert the work rate units used into watts, and explain the development of ventricular hypertrophy. Conversion factors are found in Symbols or here: 1 litre = 10-3 m3. 1 mmHg = 133.3 Pa (N/m2). 1 watt = 1 Nm/s = 1 J/s. A 59-year old office worker is known to have systemic hypertension. From the initial arterial pressure of 195/115 mmHg, he was brought down to a stable level of 160/95 mmHg by antihypertensive drugs. During work the patient suddenly collapses, and he is brought to hospital in an unconscious state with an arterial blood pressure of 75/45 mmHg. There are no signs of hemiplegia. Assume that the brain is hypoxic, and that the brain is producing lactic acid out of 30% of all glucose molecules combusted here. Among other values the blood glucose concentration is determined to 5 mM, and the arteriovenous glucose concentration difference increases to 300% of normal (0.5 mM). The cerebral bloodflow (CBF) is reduced to 50% of the normal value (650 ml min-1). The total production by oxidative phosphorylation is 36 ATP per glucose molecule, and by anaerobic metabolism 2 ATP per glucose molecule. 1. What is the most likely diagnosis? 2. Calculate the anaerobic and aerobic contribution to brain metabolism. 3. Calculate the net glucose flux and the ATP production in a normal brain, and compare the results to those of the patient. A female, 66 years of age, complains of frontal headache. She has been treated for migraine for the last 40 years. The new headache is different from migraine. The doctor measures her arterial blood pressure to 195/115 mmHg (25.9/15.3 kPa). By ultrasound screening the length of her left kidney is measured to be half the length of the right. Renal arteriography reveals a stenosis of the left renal artery. The stenosis is relieved by balloon dilatation, where a catheter with a balloon at its tip is inflated at the right site. The success of the treatment is confirmed over the following weeks, where her blood pressure reach a level of 145/95 mmHg (19.3/12.6 kPa). 1. What is the cause of her hypertension? 2. Explain the pathophysiological mechanism. 3. What is the most likely cause of her renal artery stenosis? A female, age 22 years, is sitting on a bicycle ergometer with her calf muscles 0.9 m below heart level. She is at rest and the venous pressure is 10 mmHg (1.3 kPa) at the level of the heart. The oxygen uptake(VO2) is 0.247 l STPD per min and the muscle bloodflow is 3 ml per min per 100 g of tissue (3 Flow Units, FU). The total weight of all her skeletal muscles is 30 kg. Following 5 min of rest, she starts cycling, hereby increasing her oxygen uptake to 4.5 l STPD per min, and her muscular arterioles dilatate to reach a three-fold increase in inner radius. During exercise the arterio-venous O2 content difference is 170 ml STPD per l, and the oxygen uptake in the skeletal muscles increases from 1 to 100 ml STPD per min per kg. 1. Calculate the venous pressure in the calf muscles at rest. 2. Calculate the relative alteration of the muscular vascular resistance during exercise. 3. Calculate the driving blood pressure over the working muscles during exercise, where the arterial blood pressure is 170/70 mmHg (22.7/9.3 kPa) and the venous pressure in the calf muscles is reduced to 20 mmHg (2.6 kPa). 4. Calculate the rise in muscle bloodflow during exercise. Try to solve the problems before looking up the answers. · The cardiac output(Q) is the stroke volume multiplied by the cardiac frequency. The heart must pump harder to provide a given Q° with increasing age, because the arteries become increasingly stiff with age. · The distensibility or compliance of the arterial system diminishes with age due to atherosclerosis. · When the pressure wave travels through the arterial tree, the arterial compliance is always less in the distal part of the system. · The mean arterial pressure (MAP) is a good estimate of the driving pressure (DP), whereas the pulse pressure varies almost directly with the stroke volume. · MAP and Q are easy to determine, allowing a calculation of total peripheral vascular resistance (TPVR). The systemic TPVR is one PRU at rest and 0.3 PRU during exercise. · The velocity of the systemic arterial pressure wave varies inversely with the arterial compliance, whereby the velocity increases with age and with increasing degrees of hypertension. · The high frequency components of the systemic arterial pressure wave are damped in the periphery, and the systolic peak components are elevated. · The MAP varies directly with the Q and the TPVR.. The resistance model for circulating blood: DP = Q° * TPVR is applicable for therapeutic strategies in hypertension. · The EEG of an anoxic brain is recognisable as a straight EEG trace (no electrical activity) indicating brain death. Because [Ca2+] rises in the nerve cell, this increases the K+ conductance, so that more K+ leaks out into the ISF. · The arterial blood pressure is measured indirectly in the brachial artery with Korotkoff´s auscultatory method (standardised by WHO). The systolic pressure is recorded by the occurrence of a tapping sound, and the diastolic pressure is manifested by the disappearance of the sound. · Continuous intra-arterial recordings can obtain exact arterial blood pressure measurements. Comparison with intra-arterial recordings have shown that Korotkoff´s method estimates the systolic pressure too low (about 10 mmHg), and the diastolic pressure differs a few mmHg. · A risk factor is a factor showing covariance with atherosclerosis. The remaining risk factors for atherosclerosis are physical inactivity, hypercholesterolaemia, hypertriglyceridaemia, increased LDL concentration, smoking, diabetes, and familiar factors (eg, genes, social inheritance or unhealthy life style). · Populations living under natural conditions - including Indian troops in Brazil and healthy living persons in the Western Hemisphere - maintain their mean arterial pressure (MAP) throughout life. · In the rich part of the World, the MAP and the systolic pressure, measured as an average for the total population, increases with increasing age. · Systemic hypertension - according to WHO - is defined as an arterial blood pressure exceeding 160/95 mmHg (21.3/12.6 kPa) for several months. The pressure increase is either systolic, diastolic or a combination. · Systemic hypertension is the most frequently diagnosed and treated risk factor for the development of atherosclerosis including ischaemic heart disease. · The cause of essential hypertension in the western world may well prove to be physical inactivity and related life style patterns. · Relaxed exercise is an alternative therapeutic strategy to antihypertensive drugs. Mild and relaxed motion (such as walking, bicycling, golf, jogging, swimming, badminton, tennis etc) is utilised, whenever possible, in the treatment of essential hypertension. · Mild and relaxed exercise has other beneficial effects, namely a consequential reduction of other known risk factors for atherosclerosis: Improved glucose tolerance, weight loss, improved heart function, and improved lipid profile, normal gastrointestinal functions and psychological benefits such as improved mood and a healthy sleeping pattern. · Healthy food and drinking habits are important to hypertonics, and smoking has to be given up. · A rational strategy for the future is to control the risk factors for the patients. A successful lowering of arterial blood pressure must be accompanied by improvement of other risk factors. Hypertension. Monthly journal published by the Am. Heart Association, 7272 Greenville Av., Dallas TX 75231-4596, USA. Julian DG, Camm AJ, Fox KS, Hall RJC & Poole-Wilson PA (1995) Diseases of the Heart, 2nd Edn. London: Bailliere Tindall. Katzung BG. Basic & Clinical Pharmacology. 10th Ed. Appleton & Lange, Stanford, Connecticut, 2007. Luipold G, C Zimmermann, M Mai, D Klorr, D Starck, G Gress and B Mühlbauer. Dopamine D3 receptors and salt-dependent hypertension. J. Am. Soc. Nephrol. 12: 2272, 2001
|
||
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Click here to introduce your comments or contributions