New Human Physiology | Paulev-Zubieta 2nd Edition
Chapter 21: Thermo-Regulation, Temperature and Radiation
| HOME | PREFACE | TABLE OF CONTENTS | SYMBOLS | SECTION INFO | CONTRIBUTORS | LINKS | CONTACT US |
Highlights
Study_ObjectivesPrinciplesDefinitionsEssentials
PathophysiologyEquationsSelf-AssessmentAnswers
Further Reading
|
Chapter 21
|
 |
|
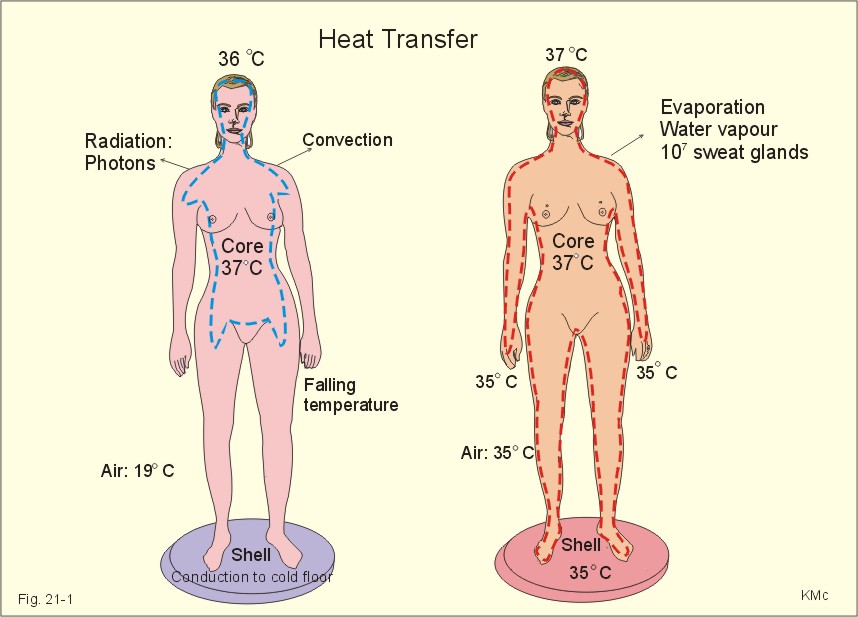
This Chapter is written following discussions with my colleague, Leif Vanggaard, MD, Arctic Institute, Copenhagen. · To define body core and body shell, heat balance, heat exchange (conduction, conversion, evaporation and radiation), hyperthermia, hypothermia, mean body temperature, heat capacity, and thermal steady state. · To describe fever (pyrogens), benignant and malignant hyperthermia, heat exhaustion, heat syncope, heat stroke, sun stroke, and hypothermia. · To describe radiation sickness. · To calculate one thermal variable, when relevant variables are given. · To explain the concepts heat exchange, thermogenesis by food and shivering, the human temperature control system and its function at different environmental temperatures. · To use the above concepts in problem solving and case histories. · Newton’s law of cooling: The dry heat loss is proportional to the temperature difference between the human body (shell) and the surroundings. · The total energy of a system is conserved in an interaction, not the kinetic energy or the mass (Einstein). If the mass changes during an interaction, there is a resultant change in kinetic energy, so that the total energy remains constant. – Heat energy is proportional to molecular movement rates – “heat energy equals movement.” · Stefan-Boltzmanns rule: The higher the temperature of an object, the more it radiates. The energy radiated from an object is proportional to the fourth power of its Kelvin temperature. – The energy radiating from an object and received by the human body is proportional to the temperature difference between the object and the skin (see Eq. 21-4). This is because human life implies relatively small temperature gradients. · Body core consists of the thermoregulated deeper parts of the body and the proximal extremity portions of warm-blooded animals including man. · Body shell refers to those outer parts of the body (skin and subcutaneous tissue) that change temperature at cold exposure. · Conductance changes of the shell are used as a measure of skin bloodflow. · Conductive heat loss describes a direct transfer of heat energy by contact between two bodies of different temperature (eg, skin and objects). · Convective heat loss is defined as the heat loss by contact between the surface (skin) and a moving medium (air or water). · Evaporative heat loss is defined as the heat loss by evaporation from the body surface or lungs. · Fever occurs when the core temperature of the body is raised above normal steady state levels. The body reacts as if it is too cold. Fever implies a disorder resulting in shivering combined with vasoconstriction, headache, dedolation, and general discomfort (eg, malaria). · Heat flow is defined as energy exchanged due to a temperature difference. Heat flow is transmitted along a temperature gradient. · Heat capacity is the amount of heat required to produce a temperature increase for a given amount of substance. · Heat energy balance in a resting person is a condition, where the heat production is equal to the heat loss. Thus the body temperature is constant and the heat storage is zero (thermal steady state). Usually, there is no internal heat energy flux between body core and shell. · Hyperthermia is an increase in core temperature above normal. · Hypothermia refers to a clinical condition with a lowered core temperature (below 35 oC). · Mean body temperature is defined according to Eq. 21-1 (see end of Chapter). · Non-shivering thermogenesis is a rise in metabolism, which is not related to muscular activity (shivering or exercise). · Insensible perspiration (leakage of the skin) is the small cutaneous evaporation loss, which is unrelated to sweat gland function. · Insulation refers to resistance to heat transfer. · Radiative heat loss is a transfer of heat energy between 2 separate objects at different temperature. Heat energy is transferred via electromagnetic waves (photons). This heat transfer does not require a medium, and the temperature of any intervening medium is immaterial. · Shell temperature is the temperature of the outer parts of the body (measured on the skin surface) and related to cold environments. · Shivering is a reflex myogenic response to cold with asynchronous or balanced muscle contractions performing no external work. · Specific heat capacity is the relationship between heat energy exchanged per weight unit of a substance and the corresponding temperature change. The specific heat capacity of water is 4.18 and of the human body (blood and tissues) 3.49 kJ kg-1 oC-1, respectively. The specific heat capacity of atmospheric air is 1.3 kJ (m3)-1 oC-1. · Temperature is the measurement of heat energy content. This paragraph deals with 1. The temperatures of the body, 2. Body responses to cold, 3. Body responses to heat, 4. Emotional sweating, 5. Metabolic Rate and environmental temperature, 6. Temperature control, 7. The human thermo-control system, and 8. Thermoregulatory effectors. 1. The temperatures of the body The human body consists of a peripheral shell and a central core (Fig. 21-1). The heat content (H or enthalpy) of the human body is reflected by its temperature. By definition a thermometer only measures the temperature of the thermometer, so its location is essential. The mean core temperature is 37 oC in healthy adults at rest, but small children have larger diurnal variations. The skin is the main heat exchanger of the body. The skin temperature is determined by the core temperature and by the environment (temperature, humidity, air velocity). Thus the shell temperature is governed by the needs of the body to exchange heat energy.
Fig. 21-1: Heat transfers, body cores and shells temperatures of a naked person standing in cold and warm air, respectively. The shell temperature is measured on the skin surface and at the hands and feet to approach the room temperature of 19oC in a person standing in a cold room for hours (Fig. 21-1, left). The shell temperature is several degrees lower than the temperature in the central core. The limbs have both a longitudinal and a radial temperature gradient. The shell temperature and the size of the shell vary with the environmental temperature and the termal state of the person. A naked person, standing on a cold floor in 19oC air has a small core and a thick shell compared to the same person in a warm environment (Fig. 21-1). The shell temperature of the skin and distal extremities is difficult to evaluate. The best estimate is measurement of the infrared heat radiation flux with a radiometer. The core temperature is the rather constant temperature in the deeper parts of the body and in the proximal extremity portions (see the red stippled lines of Fig. 21-1). However, the core temperature may vary several Centigrades between different regions depending on the cellular activity. The brain has a radial temperature gradient between its deep and superficial parts. In a sense, the temperature of the mixed venous blood represents an essential core temperature. The rectal temperature A high core temperature is found to be constant in the rectum about 10-15 cm from the anus. When measuring the rectal temperature a standard depth of 5-10 cm is used clinically. The venous plexus around the rectum communicate with the cutaneous blood in the anal region. The rectal temperature falls when the feet are cold, because cold blood passes the rectum in the veins from the legs for the same reason. The rectal temperature rises during heavy work involving the legs. Parents should be advised to measure the rectal temperature in disease suspect children. The rectal temperature is a reliable estimate of the core temperature in resting persons. Sublingual (oral) or axillary temperatures are unreliable measures of the core temperature - often more than half a degree lower than the rectal temperature. The cranial temperature (tympanic and nasal) The main control of temperature is performed by the anterior hypothalamus, which has a high bloodflow. Within the cranium the hypothalamus lies over the Circle of Willis, which supplies it with blood, and close to the cavernous sinus which drains it. Hypothalamus elicits heat loss responses when stimulated by heat. The tympanic membrane and areas in the nasal cavity (the anterior ethmoidal region, part of the sphenoid sinus) are supplied with blood from the internal carotid artery just like the hypothalamus. These cranial locations then serve as a substitute for the measurement of the inaccessible hypothalamic temperature. Intake of 250 g of ice releases an abrupt fall in the nasal temperature in a warm person, whereas the change in rectal temperature is smaller and delayed (Fig. 21-2). The cranial core temperature is more dynamic than the rectal.
Fig. 21-2: Intake of ice reduces the temperature in a warm person resting at 45oC. In sports and in surgical hypothermia dynamic measurements of core temperature are essential. The cranial temperature is often preferred. During forceful movements the thermistor may be displaced. In such situations an oesophageal location is applied at heart level. This is an approximative measure of the temperature of the mixed venous blood of the right heart located close to the thermistor. The mean body temperature is defined according to Eq. 21-1. The storage of heat energy in the body can be calculated according to its heat capacity (3.49 kJ* kg-1*oC-1), the body weight (kg) and the change in mean body temperature in the period (Eq. 21-2). According to the first law of thermodynamics, the storage of heat energy equals the metabolic energy change minus the heat loss (Eq. 21-3). Quantification of thermodynamics in humans is possible using equations 21-1 to 21-7 (later in this chapter). The body is in heat energy balance, when the storage is zero. However, the core temperature may change with internal fluxes of heat energy between core and shell without storage or loss of heat energy at a constant activity. Venous blood draining active muscles and the liver is likely to be warmer than pulmonary venous blood, since this has undergone evaporative cooling in the alveoli. A patient with high fever can be in thermal steady state, with a high constant heat production, if both core- and shell-temperatures are constant, and no internal energy flux occurs. Warm-blooded animals, homeotherms such as humans, can change their metabolism in order to keep their heat production equal to the heat loss. Such animals have a temperature control system and thereby maintain a rather constant core temperature. Warm-blooded animals live with the advantage of an unchanged cell activity and temperature in their core. However, the human core temperature falls during the oestrogen phase of the menstrual cycle and during sleep (circadian rhythm). The lowest temperature is between 18 at night and 6 o’clock in the morning (Fig. 21-3). The temperature cycle is part of the circadian periodicity. Our biological clock seems to be synchronised with the rotation of the globe. Also meals, light and temperature plays a role. Ovulation releases a sharp rise in morning temperature. Progesterone effects seem to explain the higher temperature in the last phase of the menstrual cycle (Fig. 21-3).
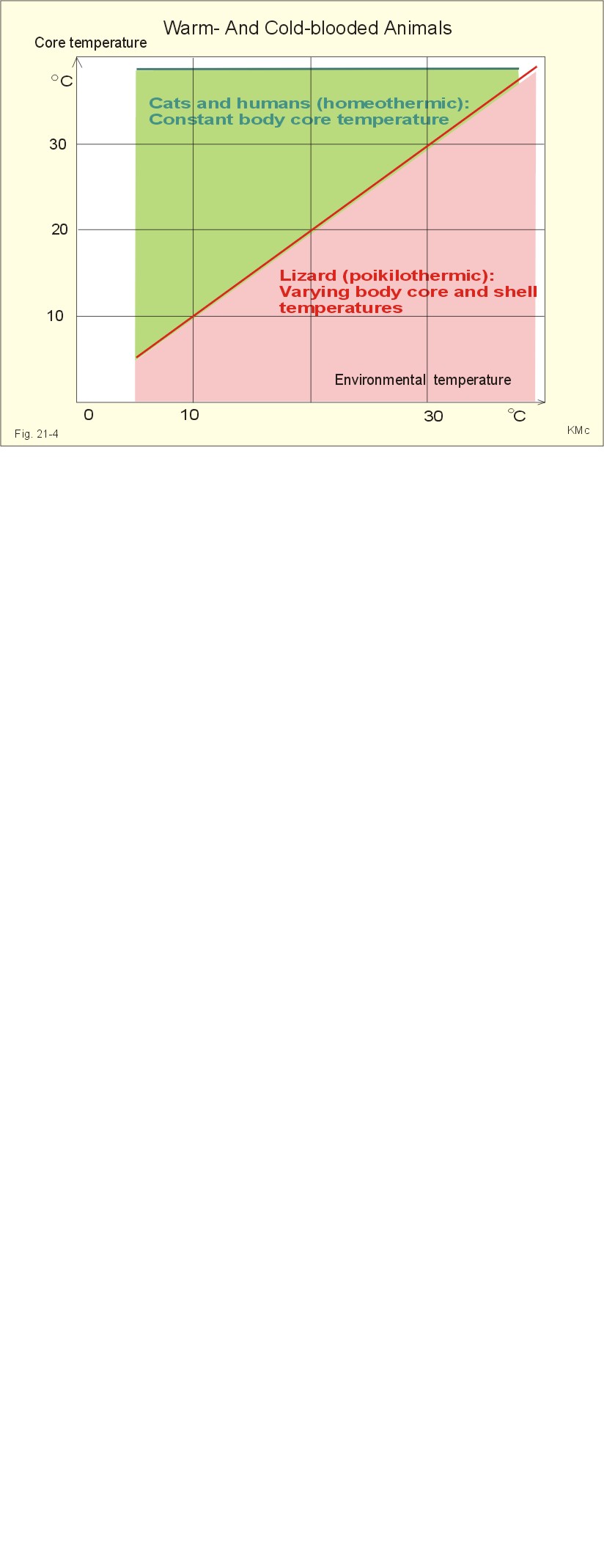
Fig. 21-3: Variations of the core temperature during 24 hour (above), and variations related to phases of the menstrual cycle (below). Cold-blooded animals (poikilotherms) live with a behavioural temperature rhythm, but have no autonomic temperature control. The core- and shell-temperatures vary with the environment and the cellular activity. Reptiles, premature and low weight-premature newborn babies are cold-blooded. These babies have no thermoregulation (see later). However, their capacity for heat production is 5-10 times as great per unit weight as that of adults. Humans have a warm-blooded (homeothermic) core and a cold-blooded (poikilothermic) shell in a cold environment. Persons exposed to general anaesthesia, alcohol, and certain drugs lose the autonomic thermoregulation. Cold-blooded animals must live with varying core and shell temperature, whereby the rate of their cellular activities varies with the surrounding temperature (Fig. 21-4).
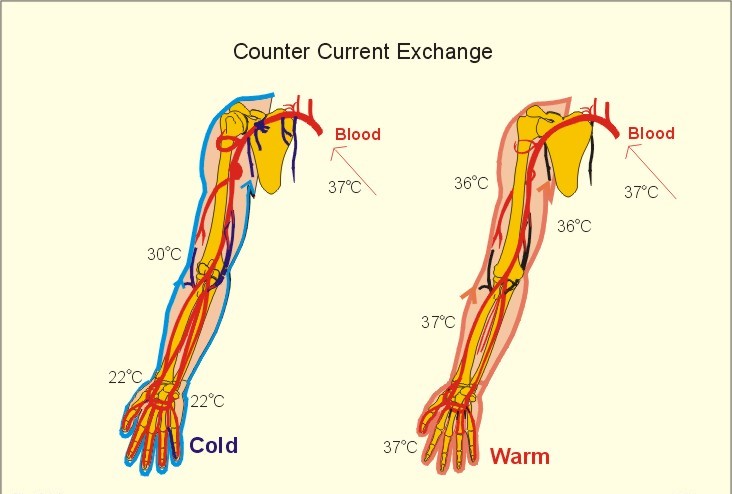
Fig. 21-4: The body core temperature and the environmental body temperature for a warm-blooded animal (cat) and a cold-blooded animal (lizard). a) Convection. The convective heat loss is calculated by Eq. 21-7. A healthy person in sports clothes experiences thermal comfort at three times the resting metabolic rate (3 MET), when the surrounding temperature is 20oC, the humidity is 50% and the wind velocity is 0.5 m*s-1. Diving (water has a high thermal conductivity) illustrates the importance of conduction andconvection in heat energy transfer. The dry diving suit excludes water from contact with the skin and traps low-conductance air in insulating clothing worn inside the watertight sealing. The wet suit traps water next to the skin but prevents its circulation. The water is warmed through contact with the skin, and the high insulation of the foam rubber wet diving suit, with its many pockets of trapped air, minimises the rate of heat energy loss to the surrounding water. Air is a poor heat conductor and thus a good insulator. During deep diving high pressures compress these air pockets and thus reduce the insulation properties of wet diving suits. b) Radiation describes a transfer of energy between objects in the form of electromagnetic waves (photons). This includes ultraviolet and visible (sun light) radiation from the outside and from the body infrared or warm heat radiation. Radiative heat transfer can be calculated for a naked person according to Eq. 21-4. When the skin temperature (Tskin) is less than the temperature of the surrounding objects, heat is gained by radiation. At wintertime, heat can be lost through a window glass by radiation from the body to the cold environment irrespective of the room temperature. This is because the skin temperature is higher than the outside temperature. c) Conduction. Sitting on a cold stone is a typical example of conduction loss, just as standing on a cold floor (Fig. 21-1). – Conduction heat can also be gained, although it is really possible to walk on glowing coals with speed and a thick epidermal horn layer. d) Evaporative heat loss- see sweat secretion below. Cutaneous vasoconstriction lowers skin temperature, and thereby reduces the conductive-convective heat loss that is determined by the temperature gradient from the skin surface to the environment. Cutaneous vasoconstriction directs the peripheral venous blood back to the body core through the deep veins and the commitant veins. These veins are located around the arteries with warm blood, so that the venous blood receives part of the heat energy from the arterial blood - so-called counter current heat exchange (Fig. 21-5). The vasoconstriction is so effective, that the bloodflow through the arterio-venous anastomoses in the fingers and toes can fall to below one percent of the flow at normal temperature. The cooling of the shell is immediate, and the size of the shell increases (Fig. 21-1). Obviously, the shell is large for a naked person in cold air. The resistance vessels of the hands may open periodically to nourish the tissues, but the high viscosity of the cold blood can endanger the tissue nutrition and result in trench foot. The arterio-venous shunts of the hands and feet are closed, so the bloodflow to the limbs is a nutritive minimum. The deep arteries and veins of the limbs lie in parallel, so the arterial bloodflow loses heat to the incoming venous blood partially surrounding the arteries (Fig. 21-5). This is a typical counter-current heat exchange. In a cold environment, where vasoconstriction and heat exchange produces cold extremities, the total insulation is increased at the expense of reduced neuromuscular efficiency.
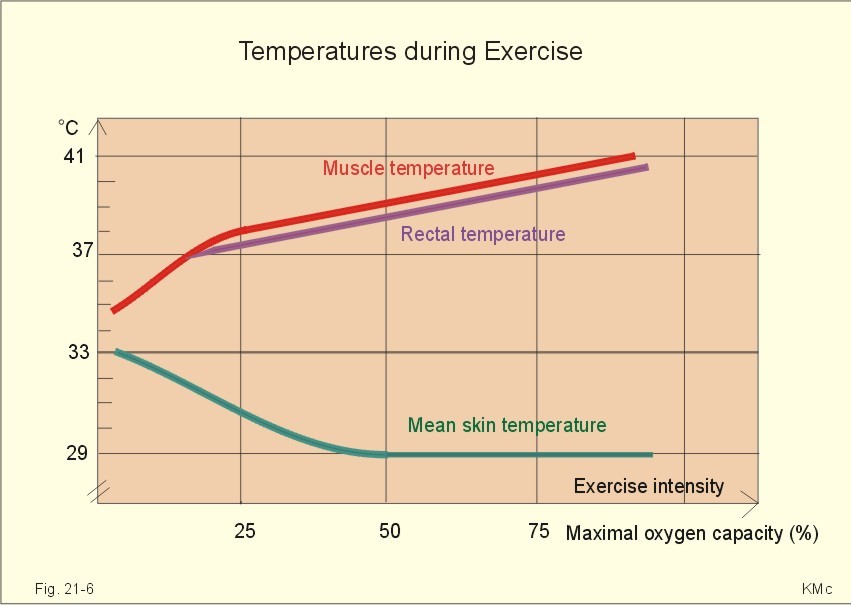
Fig. 21-5: Counter-current exchange in a human arm conserving heat energy in a cold climate (left). Superficial venous cooling ribs eliminate heat energy in a warm climate (right). In a warm climate the high bloodflow of the extremities ensures an optimal temperature of the deeper structures (eg, the neuromuscular system). The temperature of the arterial blood is maintained (Fig. 21-5, right) and the arterio-venous anastomoses are wide open conveying warm blood to the superficial veins. The superficial veins also act as cooling ribs and transfer large amounts of heat to the skin surface, where it is eliminated from the body by convection, conduction and evaporation (Fig. 21-5, right). Shivering is a reflex myogenic response to cold with asynchronous or balanced muscle contractions elicited from the hypothalamus via cutaneous receptors. The activity in agonist and antagonist muscles balance, so there is no external work. Without outside work, all energy is liberated as metabolic heat energy. Heat production is also increased by thyroid gland activity and by release of catecholamines from the adrenal medulla. External work, such as running, is helpful in maintaining body temperature when feeling cold. Cold increases the motivation for warm-up exercises and illustrates the voluntary, cortical (feedforward influence) on temperature homeostasis. The core temperature increases proportionally to the work intensity during prolonged steady state work (Fig. 21-6). The mean skin temperature falls with increasing work intensity at 20oC, because the sweat evaporation cools the skin.
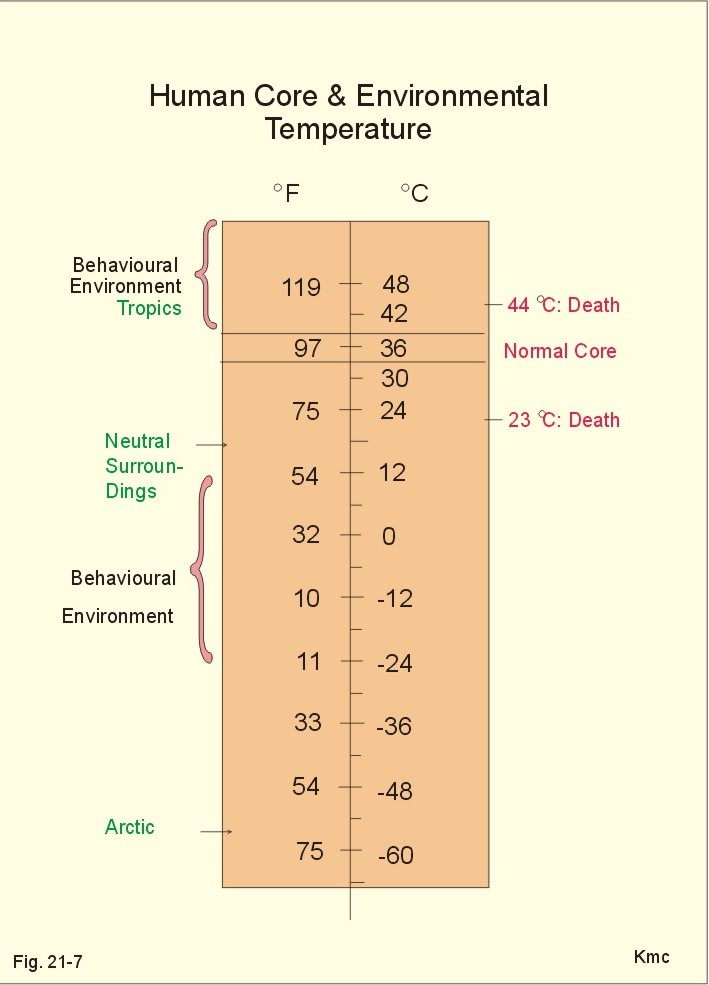
Fig. 21-6: Muscular and oesophageal temperature during steady state exercise. The levels of exercise range from zero to 100% of the maximum oxygen uptake. The temperature in the active muscles determines the level of the rectal temperature. Following marathon rectal temperatures of more than 41oC have been measured and heat strokes have occurred. A marathon is even more difficult to accomplish in warm, humid environments and strong sun may cause sunstroke (see later). People may adapt to prolonged exposure to cold by increasing their basal metabolic rate up to 50% higher than normal. This metabolic adaptation is found in Inuits (Eskimos) and other people continuously subject to cold. The environmental temperature, where we maintain our autonomic temperature control, is in the range of zero to 45oC. Below and above this range we adapt to the environment by behaviour (adding or removing clothing, warm or cold bath, sun or shadow). A core temperature above 44oC starts protein denaturation in all cells and is incompatible with life. Below 32oC humans lose consciousness and below 28oC the frequency of malignant cardiac arrhythmia’s is increasing, ending with ventricular fibrillation and death at a core temperature below 23 oC (Fig. 21-7).
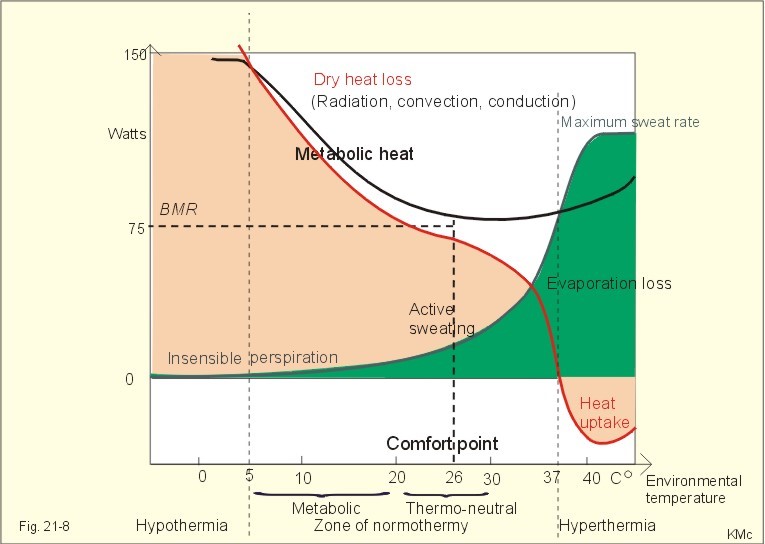
Fig. 21-7: Environmental temperature variations and temperature control. Lack of vital signs in the clinic (respiration, heart rate, EEG) must not be taken as death. Treatment must be instituted until death signs are developed. Sweat secretion. Three million sweat glands produce sweat at a rate of up to 2 litres per hour or more during exercise in extreme warm conditions. If not compensated by drinking, such high sweat rates lead to circulatory failure and shock. Sweat resembles a dilute ultrafiltrate of plasma. Healthy humans cannot maintain their body temperature, if the environmental air reaches body temperature and the air is saturated with water vapour. Primary sweat is secreted as an isosmotic fluid into the sweat duct, and subsequent NaCl reabsorption results in the final hypo-osmotic sweat. Thermal sweating is abolished by atropine, proving that the postganglionic fibres are cholinergic. Cholinergic drugs provoke sweating just as adrenergic agonists do. Evaporation of water on the body surface eliminates 2428-2436 J g-1 at mean shell temperatures of 30-32oC. Evaporation of a large volume of sweat per time unit (V°sweat) implies a substantial loss of heat according to Eq. 21-5. Normally, the skin temperature falls with increasing work intensity, because the sweat evaporation cools the skin (Fig. 21-6). Danger occurs when the average skin temperature and the body core temperature converge towards the same value. Condensation of water on the skin gains heat energy, which is stored in the body. This is what happens in a Sauna. Vasodilatation of skin vessels in warm environments results in increased cardiac output. The arterio-venous anastomoses in the hands and feet are open, and the bloodflow can rise up to at least 10 folds. The shell is minimal, when a naked person is in warm air (Fig. 21-1, right). The skin bloodflow, mainly in the extremities, determines the amount of heat energy, which is carried from the body core to be lost on the surface. The heat energy is transported from the large body core to the skin by convection in the blood. A substantial part of the heat energy is lost through the superficial veins of the extremities acting as cooling ribs (Fig. 21-5). The blood of the superficial veins is thus arterialized, when the person is warm. A piece of steak has the same composition as human skin but of course no blood flow and no sweat evaporation. Thus the steak will be cooked at an air temperature that humans can survive. A person can stay in a room with dry air at 128oC for up to 10 min during which time the steak is partially cooked. This is a paradoxical response in contrast to the thermal sweating of thermoregulation. Emotional stress elicits vasoconstriction in the hands and feet combined with profuse sweat secretion on the palmar and plantar skin surfaces. 5. Metabolic Rate and environmental temperature The total heat loss consists of the evaporative heat loss and the dry heat loss (ie, the sum of convective, conductive and radiative loss). Newton’s law of cooling states that the dry heat loss is proportional to the temperature difference between the human body (shell) and the surroundings. Let us look at a healthy, lightly dressed sitting person in thermal balance. His heat loss is plotted as the ordinate and the environmental temperature as the abscissa (Fig. 21-8). The two types of heat loss are added in order to provide the total heat energy loss. At a room temperature of 37oC there is a dry heat loss of zero, and below there is an increasing dry heat loss. Above 37oC the heat loss turns into heat input. Obviously, the dry heat loss also depends upon conduction and convection of heat inside the body by contact and by the perfusion. At extremely low environmental temperature the dry heat loss becomes larger than the metabolic heat liberation and the body is cooled down. The person is in thermal steady state, and the metabolic rate is almost constant in the thermoneutral zone between 20 and 30o C (Fig. 21-8). The law of metabolic reduction reflects the tendency for heat production to match the rate of heat loss. The thermoneutral zone, where minimal compensatory activity is required, is separated in the lower vasomotor and the upper sudomotor control zone. In the lower, comfortable zone (20-26o C) the total heat dissipation is maintained equal to the metabolic rate by cutaneous, vasomotor alterations. The small evaporation loss is termed leakage of the skin or insensible perspiration, which is unrelated to sweat gland function and rather constant at the basal metabolic rate.
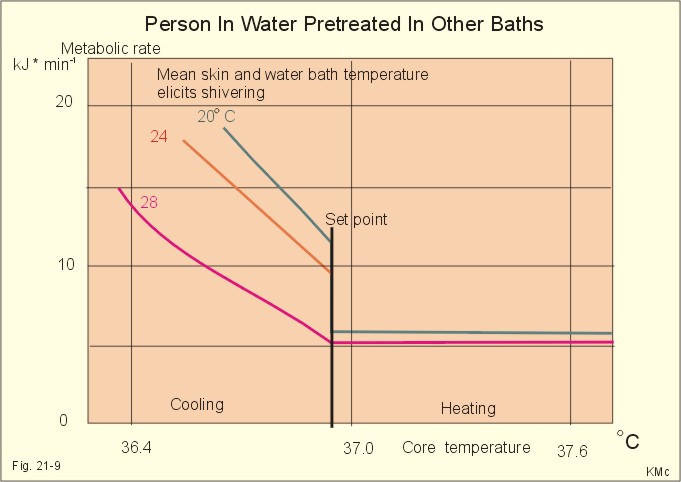
Fig. 21-8: Metabolic rate and environmental temperature in a fasting dressed human at rest. The wet and the dry heat loss, as well as the metabolic heat and the basal metabolic rate (BMR) is measured in Watts. In the upper sudomotor zone above 26o C environmental temperature, the bloodflow through the skin rises, as does sweat secretion and evaporation. At 37o C the rise in energy loss occurs via evaporation (Fig. 21-8). When the environmental temperature falls the metabolic rate increases - first by increasing muscle tone and then by shivering. The chemical or metabolic temperature control is in the environmental region from 20o C and below (Fig. 21-8), where shivering, decreased bloodflow through skin and non-myogenic heat production take place. Here, metabolism controls the core temperature by increasing metabolic rate with falling temperature in the environment. Above 20o C, the physical temperature control takes over, as an autonomic capacity for alterations in heat loss. In this thermoneutral zone the body temperature is kept constant almost without either heat-producing mechanisms or sweat secretion. - The thermal comfort for light clothed, seated persons is about an air temperature of 26oC when the humidity is 50%, 30oC for nude persons, and about 36oC sitting in water to the neck. In the metabolic zone, the total heat loss rises with falling environmental temperature, but below 5 oC in the environment, the dry heat loss exceeds the metabolic rate, and the body is cooled down (Fig. 21-8). This is the zone of hypothermia, where cold death is inevitable without treatment. The zone of hyperthermia begins at an environmental temperature of 37 oC, where humans soon reach the maximal capacity for evaporation and there is an unbalanced heat influx to the body ending in heat death. The metabolism varies with the shell and the core temperature. These relations were elucidated by series of similar experiments. A person was placed in stirred water to the neck, where the water temperature thus defined the mean shell temperature. By pre-treatment in other baths an array of core-and shell- temperature combinations were obtained and measured simultaneously with the metabolic rate (metabolic heat liberation). The core temperature was reduced by intake of up to 2 l of crushed ice in water. At a shell temperature of 20 oC, intake of ice water reduces the core temperature below 37.1 oC (here called the set point) and the metabolic rate increases by shivering (Fig. 21-9) with falling core temperature.
Fig. 21-9: The metabolic rate as a function of the core and the shell temperature. Warmer skin makes the set point fall and the rise in metabolic rate per oC (of core temperature fall) is less steep. Core temperatures above 37.1 oC all have a low metabolic rate, regardless of the shell values. At a shell temperature of 30 oC the set point decreases from 37.1 to 36.7 oC. The hypothalamus functions as a thermostat using the rest of the body to stabilise its own temperature. With rising core temperature the metabolic rate is maintained low and the body tries to cool down. When the body core temperature falls below set point, the metabolic rate increases by shivering and the heat energy storage as well. The cutaneous cold receptors are maximally active at 20 oC and they are silent above 33 oC - they can only trigger shivering, when the core temperature is below set point. Shivering ceases immediately, when we take a warm shower and the skin is warmed. The hypothalamic, preoptic heat receptors inhibit shivering, and shivering is totally blocked above the set point. Another series of experiments were directed towards heat loss. The heat loss from evaporated sweat was recorded during exercise at different shell temperatures.
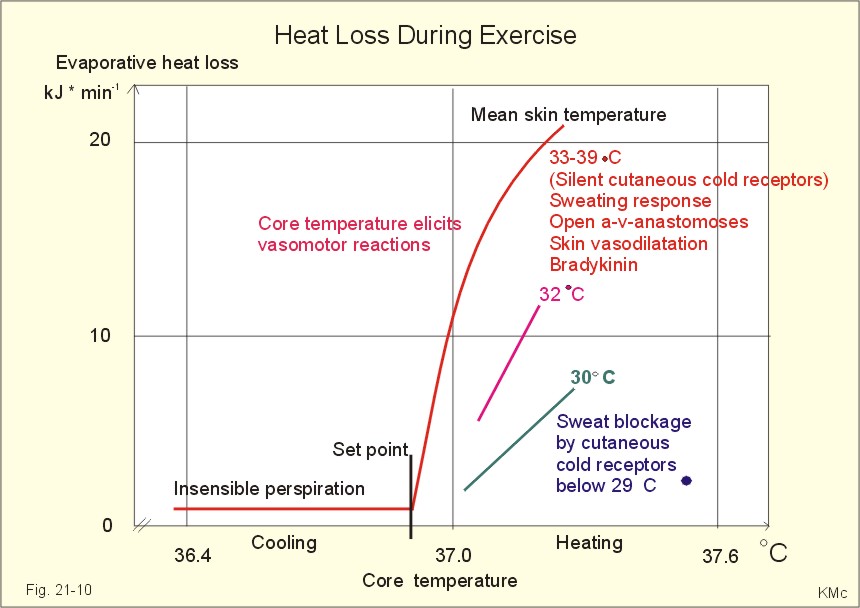
Fig. 21-10: Evaporative heat loss as a function of the core and the mean skin temperature during different intensities of exercise. Cold stimulates cutaneous cold receptors with connections to the hypothalamus (Fig. 21-12). At mean skin temperatures of 33-39 oC, where the cutaneous cold receptors are silent, the person is unable to sweat before the core temperature is above 36.9 oC (the set point of Fig. 21-10). Below the set point, the evaporation is low (perspiratio insensibilis). With increasing muscle activity and core temperature the evaporative heat loss may rise towards 20 kJ each min. Mean skin temperatures below 33 oC reduce the evaporative heat loss. The rising hypothalamic temperature releases the sweat secretion, but the local secretion is inhibited by the cutaneous cold receptors. Heat has a direct effect on preoptic heat receptors in the hypothalamus. At increased core temperature, the preoptic heat receptors totally block shivering, although the hypothalamic centre also receives shivering signals from cutaneous cold receptors in cold surroundings with mean skin temperatures below 33 oC. The falling mean skin temperature can also act directly to lower cutaneous bloodflow and sweat secretion. Humans have a rather constant core temperature although the metabolism and environmental temperature may vary considerably. This implies that control is exerted.
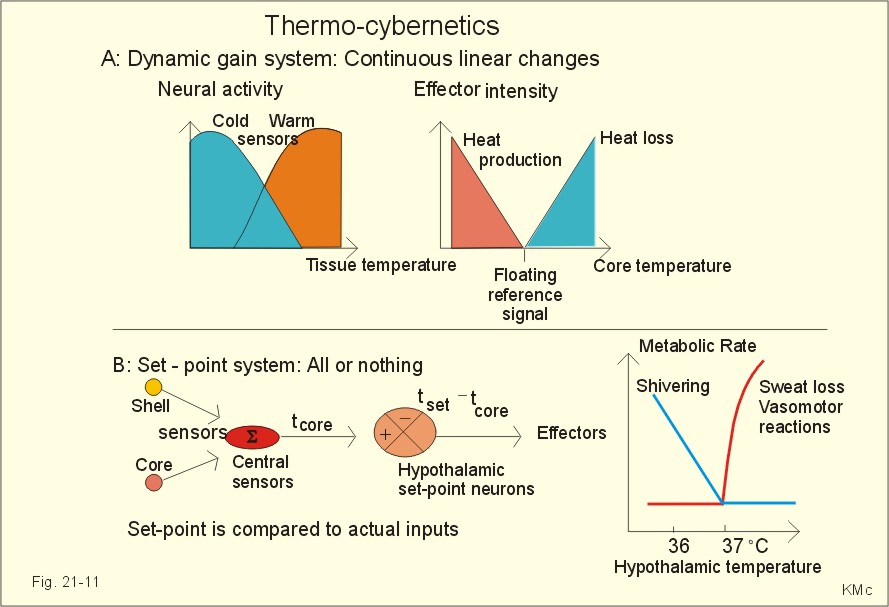
Fig. 21-11: Thermoregulation by dynamic gain and set point systems. Information about the environmental temperature is provided by peripheral thermo-sensors, which are located in the skin, abdominal organs, and muscles. Internal or blood temperature is monitored by central thermo-sensors in the preoptic hypothalamus and the medulla. A rise in hypothalamic temperature causes vasodilatation in the skin and reduces muscular tone. The person looses motivation for physical activity and reduces clothing. Then thermal sweat is observed, and after some time, reduced activity of the adrenal cortex and of the thyroid gland is also observed. A fall in hypothalamic temperature by cooling of the shell and core releases cutaneous vasoconstriction together with increased muscular tone and shivering. There is a sympathetic activation with secretion of catecholamines, oxidation of fatty acids and glucose, and increased secretion of the thyroid and adrenal gland. The muscle tone is increased, and shivering is triggered reflexly as asynchronous muscle contractions without external work (movements), so all the metabolic energy is released as heat. The capacity for muscular thermogenesis by shivering is high. Up to five folds basal metabolic rate is observed, which corresponds to heavy industrial work. Shivering may be suppressed voluntarily at the beginning. Transmission signals for shivering passes the rubrospinal pathways to a- and g-motor neurons of antagonist muscles. Dynamic gain and set point control A: A dynamic gain system responds continuously to feedback signals - regardless of the core temperature. With rising tissue temperature, the neural activity of heat sensors increases linearly, whereas the activity of cold sensors decreases (Fig. 21-11A). This combined sensory input to the hypothalamus increases the core temperature and thus increases the activity of heat loss effectors, while inhibiting heat production effectors (Fig. 21-11 A). This determines the reference signal. The dynamic gain system has a floating reference signal moving with the continuous heat loss and heat production (Fig. 21-11A). B: A set-point system does not respond to a rise in temperature before a certain set point is reached. The set point is the core temperature at which neither heat loss mechanisms or heat production mechanisms are active. When a thermal disorder reaches a certain set-point in the hypothalamus, signals passes to the effectors. The desired core temperature (tset = set point temperature) is compared to the actual value (tcore in Fig. 21-11B). The caudal hypothalamus works as a thermostat. Error signals - a deviation from tset - evoke responses that tend to restore core and hypothalamic temperature toward the set point. When the actual core and hypothalamic temperature rises above the desired set point such as 37 oC, effectors are turned on, and the compensatory heat energy loss is almost linear (Fig. 21-11B). These compensatory mechanisms (vasodilatation, sweat, reduced muscle tone) do not turn off until the temperature drops to the set point (ie, an all-or-non response). When the actual core and hypothalamic temperature is just below the set point, the compensatory mechanisms (vasoconstriction and shivering) are relatively inactive. The hypothalamic set point change with the physiological conditions and is elevated in fever by pyrogens from microorganisms. The rise in metabolism is mainly accomplished by shivering. 7. The human thermo-control system Human temperature control exhibits both dynamic gain and set point characteristics. The control system implies widespread cutaneous and deep sensors. Their afferents converge towards the hypothalamic integrator, which acts as a thermostat. The hypothalamus also contains thermosensors in the preoptic region, and inhibitory neurons perform crossing inhibition (Fig. 21-12). The central heat drive from the preoptic hypothalamus is maintained (Fig. 21-12). The stability of the core temperature is maintained by the large heat capacity of the body mass, and by the deep thermosensors, which are dominant. Shivering is released from cutaneus cold sensors firing maximally at 20 oC. These cold sensors are silent above 33 oC. The cold shell (Fig. 21-12) activates deep cold sensors in the preoptic hypothalamus. This increases heat production by shivering. The preoptic thermostat simultaneously reduces heat loss by crossing inhibition.
Fig. 21-12: The hypothalamic thermostat and its connections. Sweat secretion is released by preoptic warm sensors as soon as their temperature is 37 oC or above (tset). Cutaneous cold sensors inhibit sweat secretion at shell temperatures below 33 oC, since they are silent above this temperature. In conclusion, preoptic warm sensors show set point characteristics below the set point, and preoptic cold sensors show set point characteristics above the set point. Apart from that, preoptic sensors show dynamic gain: With rising tissue temperature, the neural activity of heat sensors increases linearly, whereas the signal frequency of cold sensors increases with falling temperature (Fig. 21-11A). Cutaneous sympathetic vasodilatation is probably also released by preoptic warm sensors above set point (Fig. 21-12). A fall in skin temperature below 33 oC will reduce skin bloodflow by crossing inhibition (Fig. 21-12). Alcohol seems to off set the thermocontrol mainly by inhibition of the hypothalamic thermostat (Fig. 21-12). Newborns, down to premature babies above 1000 g, possess certain thermoregulatory functions. The newborn can increase thermogenesis by a factor of three without shivering shows vasomotor reactions, sweat secretion, and reduces the surface area in cold air. However the baby has special problems: The surface-volume ratio is 3-fold higher than that of an adult. The baby has a thin shell due to the thin subcutaneous fat layer, so even a maximal vasoconstriction cannot limit heat loss with a capacity comparable to that of an adult. Newborns are specially equipped to perform non-shivering thermogenesis (chemical thermogenesis). Non-shivering thermogenesis is any rise in metabolism, which is not related to shivering. In babies this form of thermogenesis is particularly large in their brown adipose tissue. This tissue is abundant around vital organs, in neck and mediastinum, between scapulae and in the armpits. Brown adipose tissue cells contains multilocular droplets in the fat phase and many mitochondria. The tissue receives sympathetic innervation and is stimulated by catecholamines and thyroid hormones. Cooling increases the bloodflow and temperature of brown adipose tissue. Noradrenaline injections cause vasodilatation via b-receptors, and increase the metabolism to the same extent. The cause of the increased metabolism is an increased cell membrane permeability for Na+- and K+-ions, whereby the Na+- K+-pump (high ATP demand) is activated.
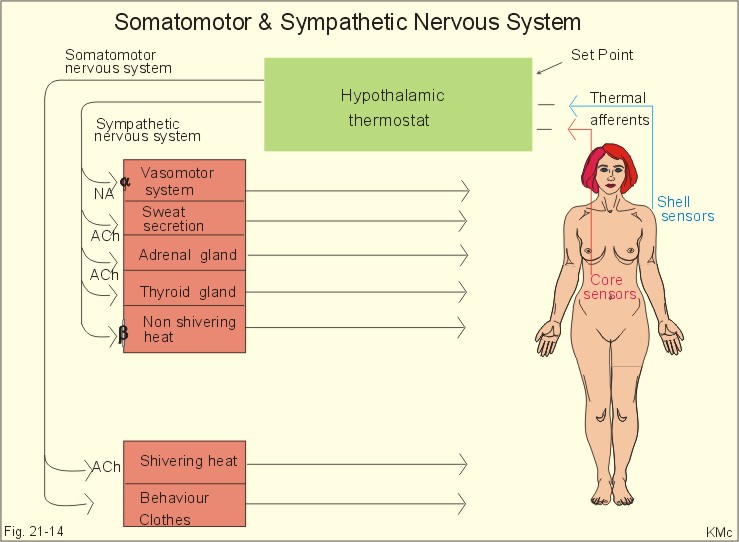
Fig. 21-13: Thermocontrol in the newborn. Newborns are in thermal balance at a minimal metabolism only when the surrounding temperature is high (32-34 oC). With other words, newborns have an extremely high lower threshold for the thermoneutral zone, namely 32 oC. The threshold for maximal use of shivering is approximately 23 oC compared to a naked adult about 5 oC. In general, these threshold values for newborn increase with falling body weight in premature. Premature below 1000 g has hardly any thermoneutral zone (Fig. 21-13). They are actually cold-blooded and their temperature control is maintained with a couveuse. The sympathetic and the somatomotor nervous system participate in thermoregulation (Fig. 21-14). Noradrenergic sympathetic neurons control the bloodflow through fingers, hands, ears, lips and nose. Arterioles contract and arteriovenous anastomoses close (thermal insulation) following an increase in sympathetic tone, and dilatate following a decrease in tone. When arterioles and arteriovenous anastomoses open, the bloodflow is markedly increased and thus the convective heat loss from the skin is increased.
Fig. 21-14: The thermoregulatory feedback system. Cholinergic sympathetic fibres control sweat secretion. The vasodilatator bradykinin is liberated in the skin. Thus, profuse sweat secretion is always accompanied by vasodilatation. Sympathetic activation releases thyroid hormones from the thyroid gland and catecholamines from the adrenal medulla. These hormones liberate fatty acids and glucose for combustion. A reduced sympathetic tone also reduces the activity of the adrenal and the thyroid gland. The thermogenic response to cold also involves a non-myogenic or non-shivering component probably in adipocytes. Non-shivering heat production is controlled by the sympathetic nervous system via adrenergic b-receptors. The noradrenaline (NA in Fig. 21-14) released at the nerve terminals close to the adipocytes, stimulates the liberation of free fatty acids and their subsequent oxidation. Non-myogenic heat production includes a contribution from the brown fat of babies, but is insignificant in adults. Shivering is induced by way of the motor system. The central shivering pathway passes from the hypothalamus to the motor neurons in the spinal cord. Shivering is abolished by blockade of the neuromuscular end plate with curare. Thermoregulatory behaviour such as fanning and adding or removing clothing is effective in changing the thermal insulation. Several layers of clothing with trapped air act as a good insulator. In healthy persons, heat energy is liberated from cellular metabolism and transferred to the environment through the skin by sweating and vasodilatation. Sweating occurs during exercise, and its evaporation is the most important mechanism in maintaining the core temperature as close to 37o C as possible. The thermoregulatory centre in the hypothalamus controls all processes.
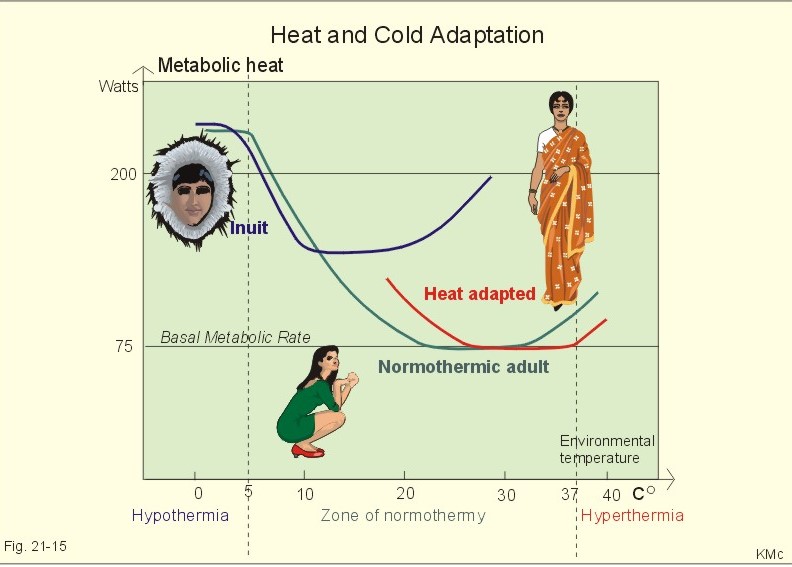
Fig. 21-15: Heat and cold adaptation Cold adaptation is found among Australian aborigines and Inuits in Greenland. Inuits have relatively more sweat glands in the face and less on the body. Aborigines can sleep naked on the ground even at low temperature. Inuits have a basal metabolic rate 50% higher than persons living in a temperate climate do. The threshold for shivering is shifted towards the left in cold-adapted persons, but they maintain normal function at the new set point. Very old people may show the same phenomenon, and live with a core temperature of 35 oC without shivering. Obviously, cold adaptation implies non-shivering thermogenesis, which is oeconomic metabolic heat liberation (Fig. 21-15). Heat acclimatization is actually a sweat gland adaptation, and a 2-week process following arrival to a hot climate such as the tropics or a desert. Gradually sweat-evaporation is increased and the NaCl loss is reduced. The sweat secretion capacity may reach 4 l each hour with a thin sweat. The adaptation is caused by increased aldosterone secretion from the adrenal cortex. Aldosterone increases the reabsorption of NaCl and the secretion of K+ from the sweat, during its passage of the sweat gland tubules. The larger sweat loss the thirstier one feels. This is because the large sweat secretion reduces the time period for NaCl- reabsorption in the sweat gland tubules. The resulting high NaCl concentration in the plasma implies thirst, so heat adapted persons have to drink a lot. Thirst is an extremely late indicator of dehydration during work in a warm climate. Tropic inhabitants are of course heat-adapted. They have an increased core temperature (set point) and their threshold for sweat and vasodilatation is typically 0.5oC higher than that of a person living in the temperate zone (Fig. 21-15). This paragraph deals with 1. Heat cramps, 2. Heat exhaustion and heat stroke, 3. Malignant hyperthermia, 4. Hypothermia, 5. Frostbite, and 6. Fever and hyperthermia. A paragraph concerning nuclear energy radiation is given at the end. Painful cramps in the leg muscles occur following exercise, when athletes run too fast in a hot climate. Heat cramps respond to salt and water replenishment in a normal diet, and the cramps are probably caused by hyponatraemia. During prolonged sweating, the runner is losing salt and water. If only the water loss is replenished, the result is water-induced hyponatraemia - a parallel to the classical miner’s cramps. 2. Heat Exhaustion and Heat Stroke When the water-salt balance is at risk in a hot climate, it is always a threat to the circulation. Profuse sweat secretion, in a subject who is not acclimatized, results in salt- and water depletion, with a daily loss of more than one mol of NaCl and more than 6 l of water. Within a period of one-hour strenuous working endurance athletes have lost up to 8 l of water. The falling extracellular fluid volume and increasing body and brain temperature to above 40oC elicit severe symptoms and signs. As the volume and salt depletion develops, the sweat production goes down in spite of extreme vasodilatation. The falling blood pressure stimulates the high-pressure baroreceptors resulting in a rising heart rate. The dehydration with imminent shock frequently results in cerebral, renal and hepatic failure. The low brain bloodflow through an overheated brain leads to fatigue (heat exhaustion), confusion and unconsciousness or syncope (heat syncope). The confusion may develop into a veritable delirium (an acute impairment of consciousness) with brain oedema. Heat stroke - in the sun it is called sunstroke - is heat collapse that occurs suddenly, hereby creating a life-threatening condition. This heat collapse often occurs in warm, humid environments, when an unacclimatized subject exercises. The subject - without sweating (hypothalamic failure) -suddenly falls into coma, if not preceded by a short period of confusion and delirium. The condition is fatal, if not relieved by rapid cooling. Malignant hyperpyrexia is often caused by a genetic defect (autosomal dominant) in the sarcoplasmic reticulum of skeletal muscles. General anaesthesia (often halogen-substituted ethane) triggers an allergic reaction with sudden opening of Ca2+ - channels in the muscle cells. The following influx of Ca2+ elicits generalized and maintained muscle contraction (rigidity), which liberates enormous quantities of heat energy. This condition is life threatening and often results in sudden death during or just after anaesthesia. Hypothermia is a fall in core temperature to values below 35 oC. Hypothermic subjects lose consciousness, when the core temperature falls below 32 oC - a potentially lethal condition called severe hypothermia. During anaesthesia and surgery the core temperature of the patient falls and stabilise around 34-35 oC after 4-5 hours. Such a surgery hypothermia increases the risk of cardiac complications, bleeding tendency and prolonged wound healing. The condition is a prominent cause of death in climbers and skiers, as well as in persons being immersed in cold water or living in the Antarctis. The climbers and skiers are often exposed to a cold, wet and windy environment carrying insufficient clothing. As the neuromuscular function suffers, they can no longer move. General hypothermia develops and they die. In mild hypothermia the subject can still take action to rewarm by exercise and clothing, but as consciousness is lost the core temperature falls further, because shivering is abolished. The patient feels cold to touch, is in a developing coma, the circulation and respiration fall, as does the metabolic rate. The dissociation curve of oxyhaemoglobin is moved to the left, and the solubility of gasses increases as the blood temperature falls. The heart is the target organ in hypothermia. Below 30 oC, spontaneous remission is practically impossible, and death ensues from ventricular fibrillation occurring around 28 oC. Careful monitoring of all vital functions is required during rewarming, which is performed either passively (rewarming by the patients own metabolism) with insulation and space blankets or actively by a warm water bath, while monitoring the patient. A good strategy in treating hypothermic victims is the slogan: “They are not dead until they are warm and dead.” An arterial blood sample from a hypothermic patient is routinely analysed at 37 oC. The PaO2 and pHa is falsely higher, the PaCO2 is falsely lower, than in the circulating blood of the hypothermic patient. This is because more CO2 is bound also as carbamino-haemoglobin, and less O2 is bound in the cold blood. Base Excess is defined at 37 oC and thus a true metabolic variable (see Chapter 17). Artificially induced hypothermia is used in brain- and heart-surgery, where the usual thermocontrol is inactivated by general anaesthesia. The procedure becomes dangerous, when it elicits ventricular fibrillation. Frostbite is a local cold injury due to the formation of extracellular ice crystals in the skin and other tissues. This leads to extracellular dehydration and hyperosmosis, whereby the cells lose water until they die. As the skin temperature falls below + 7 oC the subjects have lost their sensory functions, and thus do not recognise the developing frostbite. The most effective treatment is warming of the still frozen area by immersion in 40-42 oC hot water following hospitalisation. The patient experiences severe pain (above + 7 oC) and morphine must be administered. Tissue which is no longer frozen must be treated sterile. Fever occurs when the core temperature of the body is raised above normal steady state levels. The body reacts as if it is too cold, while the temperature rises up to the new higher set point. Fever attacks imply shivering combined with vasoconstriction, headache, dedolation pains, and general discomfort. Fever is the result of one of two phenomena: the set point may be set to a higher level, or the efficacy of the temperature control system may be impaired. Fever implies hyperthermia; however many cases of hyperthermia do not constitute fever. Fever results from the action of endogenous pyrogens on the hypothalamic heat control centre (they increase the set point for the core temperature via prostaglandins). Exogenous pyrogens from microbes cause these endogenous polypeptides to be released from the defence cells of the body (ie, the reticuloendothelial system, RES). Antipyretic drugs inhibit cyclo-oxygenase activity, hereby interfering with the synthesis of prostaglandins and thromboxanes. Following an attack of fever, vasodilatation and sweat evaporation reduces the core temperature. Physiologic hyperthermia is an increase in core temperature caused by extreme heat stressor exercise. During work the body temperature rises up to 39oC without clinical consequences.Hereby, the heat loss capacity is exceeded. During hyperthermia the heat loss effectors are strained to the utmost. The high body temperatures of exercise activate cooling mechanisms and elicit sweat loss, which strive to return the core temperature to its normal level.In extreme hyperthermia the core temperature may rise to more than 41o C (heat stroke). Irreversible protein denaturation occurs above 44oC with brain oedema and destroyed thermoneurons in the hypothalamus. Clinically, the brain damage is shown with disorientation, lack of sweat secretion, delirium and universal cramps before death. Ionizing radiation implies destruction of tissue molecules. Dosages of absorbed radiation is measured in Joules per kg (1 J kg -1 is known as a gray, Gy). One Gy is equivalent to 100 rads. Radioactivity is measured as the number of degradations per second in bequerels or Bq. One degradation per s from radioactive material equals one Bq. The absorbed dose of radiation is balanced for damaging ionizing tissue effect, since different types of radiation have different density of ionization. A dose equivalent termed sievert (Sv) causes a rather large damage. The annual background radiation is 2.5 milli-Sv (2.5 mSv). Non-penetrating radiation occurs from alpha- and beta particles. These particles are stopped by paper, but when they enter a tissue - such as the bone marrow – they stay there and spoil everything. Penetrating radiation consists of either gamma rays (neutron) or X-rays. Survivors from nuclear power plant accidents, with whole body absorption greater than 100 rads, are threatened by acute and chronic radiation sickness. Acute radiation sickness appears as vomiting and malaise following exposure to 1 Gy (100 rad) or more. Lymphocyte production is reduced immediately, soon followed by leucopenia and thrombocytopenia with bleeding. The villi of the gastrointestinal tract are destroyed, absorption of nutrients is impaired, and new villous cells are not produced. Diarrhoea, often with blood loss, results in dehydration and anaemia. The skin is red and blistering, and the hair is loosed. The immunodeficiency system is destroyed, and secondary infections have a high mortality - especially pulmonary infections. Cerebral oedema may kill the victim within hours when exposed to 35 Gy or more. Contamination with radioactive iodine is treated by immediate intake of potassium iodide, which block the major part of the thyroid absorption. The treatment of seriously exposed radiation victims is supportive and frustrane. Chronic radiation sickness or late radiation damage implies an increased rate of mutagenesis, which includes a high frequency of leucaemia, cancer of the brain, the thyroid and the salivary glands, infertility and cataract (ie, an eye disease where the vision is blurred by an opaque lens). The radiation liberates large amounts of highly reactive ions in the cells. The reactive ions rupture DNA strands and cause mutations with production of cancer cells. Cancer cells multiply exponentially and their energy demand approach the total nutritive energy available, causing malnutrition and death. The nuclear power plant accident in Tjernobyl, Ukraine, had many victims from radiation exposure. The nearby town, Pripatja, previously with 40,000 residents is now abandoned. The frequency of thyroid cancer among children in Ukraine is more than 100 times the expected. Most of the children and young persons exposed have developed leucaemia or cancer. Their airway epithelium and respiration is seriously affected, and they have an unusual high frequency of cerebral haemorrhage. · The mean body temperature (Tbody) is calculated with the following equation: Eq. 21-1: Tbody = (0.7 × Tcore + 0.3 × Tshell), where the mean shell temperature (Tshell ) is estimated from a series of representative skin temperatures. The obvious assumption in this equation is that 70% of the body weight is core (Tcore), and the balance is shell, but the size of the shell varies with the environmental temperature. · The storage of heat energy in the body is calculated as follows: Eq. 21-2: DH STORE = 3.49*BODY WEIGHT* (T2 - T1) with the unit kJ per hour. · According to the first law of thermodynamics, the following relation is valid: Eq. 21-3: DH STORE = DH METABOLIC - (DH RADIATION +DH CON + DH EVAPORATION ) where DH CON is the change in heat loss by convection and conduction. · Radiative heat loss from a warm object (Tobj ) can be calculated for a naked person with a known skin temperature (Tskin ): Eq. 21-4: DH RADIATION = 0.5 × A × (Tskin - Tobj) where 0.5 is kJ min-1 m-2 K-1, A is the area of the human body (radiating or receiving radiation), and Tobj is the temperature of the object exchanging energy. This equation is an approximation of Stefan-Boltzmanns rule. · Evaporation of water on the body surface eliminates 2430 J g-1. Evaporation of large volume rates of sweat (V°sweat) implies a substantial loss of evaporative energy (J/min) according to the equation: Eq. 21-5: DH EVAPORATION (J min-1) = 2430 (J g-1) × V°sweat (g min-1). · Changes in heat conduction through the shell (conductanceshell) reflect changes in skin bloodflow. The conductance can be calculated by the formula: Eq. 21-6: Conductanceshell = Metabolic Rate/(Tcore - Tshell). A large temperature difference implies an effective isolation, whereas a small difference implies a low isolation capacity. · The heat loss of a naked person resting in quiet air by convection (including a minor part by conduction without movement) is given by the following equation: Eq. 21-7: HCON = 0.5 *(Tshell - Tair) in kJ per min. This equation is an approximation of Newton’s law of cooling. Each of the following five statements have True/False options: A. Humans can survive at a temperature that would cook a piece of steak, because the steak cannot dissipate core heat energy. B. Heat conductance of air at high pressure exceeds that at low pressure, whereby more heat energy is lost from the divers body by conduction through air inside a diving bell deep under water than at one atmosphere of pressure. C. Temperature homeostasis is present when heat energy production equals heat loss. D. Basal metabolic rate (BMR) is lower before than after a meal. E. The neutral environmental temperature defines the level, where the resting metabolic rate is minimal. II. Each of the following five statements have True/False options. A. Water-induced hyponatraemia is called miners cramps. B. Substantial influx of Ca2+ to the cells is probably involved in some cases of malignant hyperthermia. C. Hypothermia is a fall in core temperature below 32oC. D. One degradation per second from radioactive material equals one bequerels (1 Bq), which is also equal to one curie. E. Acute radiation reduces leucocyte and thrombocyte production. A male with a body weight of 70 kg stops his malaria prophylaxis with primaquine when leaving the endemic area. Three weeks later, a sudden attack of fever increases his core temperature from 37 to 40oC within 30 min. The heat capacity of the human body is 3.47 kJ/kg and per oC. The metabolic rate of the subject increased substantially during the rise in temperature. Following the cold stage with uncontrollable shivering, the patient develops a delirious condition with severe headache. Two hours later the patient develops a profuse sweating. Partially evaporation of the water in 32 ml sweat/min (25% evaporates) occurs from the body surface (eliminating 2,436 J/g), during which body temperature drops. Calculate the extra heat energy stored in his body after 30 min. 1. Calculate the smallest possible metabolic rate in the 30-min period. 2. What causes the extra heat energy stored in the body? 3. Calculate the reduction in body temperature by ingestion of one L of ice water, when the fever is at its highest level. 4. Calculate the time it takes to lose the accumulated heat energy by evaporation. A male sedentary person, weight 70 kg, has a daily food intake of 400 g carbohydrate (17.5 kJ/g), 100 g fat (39 kJ/g), and 100 g protein (17 kJ/g). There is a metabolic water formation of 32 mg/kJ. The man excretes 2100 ml of water (i.e., 1200 ml in the urine, 100 ml in faeces, and 800 ml through lungs and skin). 1. Calculate the metabolic rate (in kJ/day or MJ/day). 2. The man is in water balance by a water intake of 1,700 ml as a total. Explain this apparent imbalance. A 79-year old male is found apparently dead in the snow following a winter storm, where all traffic was arrested by snow. His muscles are stiff, and the heart rate is not palpable. The tendon reflexes are depressed, and the pupillary and other brainstem reflexes are lost. The body is placed in a chapel at the hospital until the funeral. The next day the personnel are disturbed by noises from the chapel. Obviously, the man is alive. 1. What has awakened the man? 2. Suggest a likely core temperature, at the time where the man was admitted to the hospital. A 20-year old person, with a body surface area of 1.8 m2, is at rest with a metabolic rate (MR, or heat energy production and transfer) of 80 Watts. His rectal temperature is 37 oC and his mean skin temperature is 33 oC. - Suddenly, a malaria attack develops with a 7-fold rise in MR, and the patient reach a temperature plateau of 40 oC, with a mean skin temperature of 34 oC. The conductance of the shell (Cshell) is a measure of skin bloodflow. This can be calculated by the formula: Cshell = MR/(Tcore - Tshell ). 1 Calculate the conductance of the shell at rest. 2. Calculate the conductance of the shell at the fever plateau. 3. How does the body accomplish this increase? Try to solve the problems before looking up the answers.. · The core temperature is 37 oC in healthy adults at rest, but small children have larger diurnal variations. · Parents should be advised to measure the rectal temperature in disease suspect children. The rectal temperature is a reliable estimate of the core temperature in resting persons. · A constant core temperature does not guarantee heat energy balance, because the energy content of the shell may change with the surroundings. · The human core temperature falls during the oestrogen phase of the menstrual cycle and during sleep. The lowest temperature is between 18 at night and 6 o’clock in the morning. Progesterone effects seem to explain the higher temperature in the last phase of the menstrual cycle · The temperature cycle is part of the circadian periodicity. Our biological clock seems to be synchronised with the rotation of the globe. Also meals, light and temperature plays a role. · The thermal comfort point for light-clothed, seated persons is about 26oC when the humidity is 50%, 30oC for nude persons, and about 36oC sitting in water to the neck. · Vasodilatation in warm environments permits increased skin bloodflow as the cardiac output also begins to rise. The arterio-venous anastomoses are dilatated, and the bloodflow can rise to at least 10 folds in hands and feet. · In the metabolic zone, the total heat loss rises with falling temperature, but below 5 oC the dry heat loss exceeds the metabolic rate, and the body is cooled down. This is the zone of hypothermia, where cold death is inevitable without therapy. · Sweat secretion. Three million sweat glands produce sweat at a rate of up to 2 litres per hour or more during extreme conditions. Such high sweat rates lead to circulatory failure and shock. Sweat resembles a dilute ultrafiltrate of plasma. · The zone of hyperthermia begins at an environmental temperature of 37 oC in humid air, where we soon reach the maximal capacity for sweat secretion, and there is a heat influx to the body ending in heat death. · The hypothalamus functions as a thermostat using the rest of the body to stabilise its own temperature. · A dynamic gain system responds continuously to feedback signals, regardless of the size of the core temperature. With rising tissue temperature, the neural activity of heat sensors increases linearly, whereas the activity of cold sensors decreases · A set-point system does not respond to a rise in temperature before a certain set point is reached. The set point is the core temperature at which neither heat loss mechanisms or heat production mechanisms are active. · Human temperature control exhibits both dynamic gain and set point characteristics. The control system implies widespread cutaneous and deep sensors. Their afferents converge towards the hypothalamic integrator and thermostat. · The thermogenic response to cold also involves a non-myogenic or non-shivering component probably in adipocytes. Non-shivering heat production is controlled by the sympathetic nervous system via adrenergic b-receptors. · Non-shivering thermogenesis is any rise in metabolism, which is not related to muscular activity. In babies this form of thermogenesis is particularly large in their brown adipose tissue. The brown adipose tissue of babies is abundant around vital organs, in neck and mediastinum, between scapulae and in the armpits. · Newborns are in thermal balance at a minimal metabolism only when the surrounding temperature is high (32-34 oC). · Thermoregulatory behaviour such as fanning and adding or removing clothing is effective in changing the thermal insulation. Several layers of clothing with trapped air are good insulators. · Heat acclimatization is actually a sweat gland adaptation, and a 2-week process following arrival to a hot climate. Gradually sweat-evaporation is increased and the NaCl loss is reduced. The adaptation is caused by increased aldosterone secretion from the adrenal cortex. · Hypovolaemia with low brain bloodflow through an overheated brain leads to fatigue (heat exhaustion), confusion and unconsciousness or syncope (heat syncope). The confusion may develop into a veritable delirium with brain oedema. · Heat stroke - in the sun called sunstroke - is heat collapse with high brain temperature that occurs suddenly, hereby creating a life-threatening condition. · Hypothermia is a fall in core temperature to values below 35 oC. Hypothermic subjects lose consciousness, when the core temperature falls below 32 oC - a potentially lethal condition called severe hypothermia. · Artificially induced hypothermia is used in brain- and heart-surgery, where the usual thermocontrol is inactivated by general anaesthesia. · Penetrating radiation consists of either gamma rays (neutrons) or X-rays. Survivors from nuclear power plant accidents with whole body absorption greater than 100 rads are threatened by acute and chronic radiation sickness. · Acute radiation sickness appears as vomiting and malaise following exposure to 1 Gy (100 rad) or more. Lymphocyte production is reduced immediately, soon followed by leucopenia and thrombocytopenia with bleeding. The villi of the gastrointestinal tract are destroyed, absorption of nutrients is impaired, and new villous cells are not produced. Diarrhoea, often with blood loss, results in dehydration. The skin is red and blistering, and the hair is loosed. · Chronic radiation sickness or late radiation damage implies an increased rate of mutagenesis, which includes a high frequency of leucaemia, cancer of the brain, the thyroid and the salivary glands, infertility and cataract. Scientific American. Monthly journal published by Scientific American Inc., 415 Madison Avenue, N.Y., USA. Benzinger, T. H. "The human thermostat." Sci. Am. 204: 134-147, 1961. Hong, S. K. News in Physiol. Sci. 2: 79, 1987. Wasserman, D.H. and A.D. Cherrington. "Hepatic fuel metabolism during muscular work: Role and regulation." Am. J. Physiol. 260: E811, 1991.
|
||




.jpg){kind=link}
Click here to introduce your comments or contributions