New Human Physiology | Paulev-Zubieta 2nd Edition
Chapter 18: Exercise, Sports and Doping
| HOME | PREFACE | TABLE OF CONTENTS | SYMBOLS | SECTION INFO | CONTRIBUTORS | LINKS | CONTACT US |
Highlights
Study_ObjectivesPrinciplesDefinitionsEssentials
PathophysiologyEquationsSelf-AssessmentAnswers
Further Reading
|
Chapter 18
|
 |
|
|
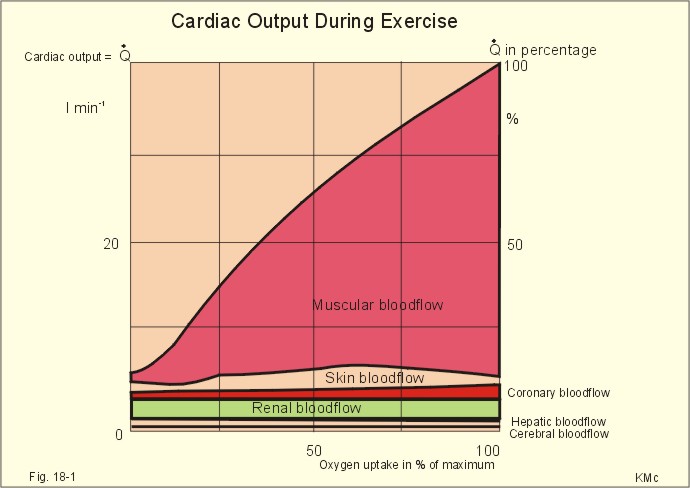
· To define factors of importance to oxygen uptake, cardiac output, and ventilation during exercise. · To describe the rise in ventilation, oxygen uptake and cardiac output during increasing exercise intensity, the concepts anaerobic threshold, oxygen deficiency and oxygen debt. · To calculate the relationship between the major variables. · To explain the metabolism and limits of exercise, typical sport injuries, doping, the effects of training including health consequences, and hypotheses of the cardiopulmonary regulation. · To use the concepts in problem solving and case histories. · The human body has a redundancy of overlapping cardio-pulmonary control systems during exercise. · The redundancy-hypothesis, with neural factors dominating at the start of work and peripheral feedback control during steady state, is a possible explanation of the hyperpnoea of exercise and the related increase in cardiovascular activity . · Anaerobic threshold. This is the exercise level above which the energy requirements can be satisfied only by the combined aerobic metabolism and anaerobic glycolysis. Lactic acid is produced and stimulates the peripheral chemoreceptors. Hereby, ventilation starts to increase out of proportion to the rise in oxygen uptake. · Blood doping. Blood boosting is an artificial improvement of performance through an increase in the haemoglobin binding capacity. Blood doping (one litre) definitely improves the oxygen transport with the blood and also the maximal oxygen uptake, which is beneficial to distance runners. · Doping: Athletes who use drugs or other means with the intention to improve performance artificially are doped by definition. · Endurance capacity or fitness number is given as the maximal oxygen uptake in ml of oxygen STPD min-1 kg-1. · Energy equivalent of oxygen on a mixed diet is defined as the heat energy liberated in the body per litre of oxygen used (20 kJ of energy per litre at an RQ of 0.8). · Flow Units (FU) measure relative bloodflow as the number of ml of blood passing an organ per 100 g of tissue and per min. · Mean Arterial Pressure (MAP) is the arterial blood pressure measured as the sum of the diastolic pressure plus 1/3 of the pulse pressure (see below). · Mechanical efficiency is the ratio between external work and the total energy used during work. · Oxygen debt is defined as the extra volume of oxygen that is needed to restore all the energetic systems to their normal state after exercise. · Oxygen deficiency is defined as the difference in oxygen volume between an ideal, hypothetical oxygen uptake and the actual uptake in real life. The missing oxygen volume at the initiation of exercise is the oxygen deficit. · Pseudo-doping. Many drugs reputedly increase athletic performance, but the fact remains that such effects rarely show up in double-blind controlled trials. - On the contrary, serious side effects occur with a biologically high and statistically significant frequency. This paragraph deals with 1. Athletes and training, 2. Fitness testing, 3. Limits of exercise performance, 4. The anaerobic threshold, 5. Ventilation and oxygen uptake, 6. Cardiopulmonary control, and 7. Oxygen debt and deficiency. At the start of exercise, signals from the brain and from the working muscles bombard the cardiopulmonary control centres in the brainstem. Both cardiac output and ventilation increase, the a-adrenergic vasoconstrictor tone of the muscular arterioles falls abruptly, whereas the vascular resistance increases in inactive tissues. The systolic blood pressure increases, whereas the MAP only rises minimally during dynamic exercise. The total peripheral vascular resistance (TPVR) falls during moderate exercise to 0.25-0.3 of the level at rest, because of the massive vasodilatation in the muscular arterioles of almost 35 kg muscle mass. This is why the major portion of cardiac output passes through the skeletal muscles (Fig. 18-1) and why the diastolic pressure often decreases during exercise. The coronary bloodflow increases, and at some intensities of exercise we see increases in the skin bloodflow (Fig. 18-1).
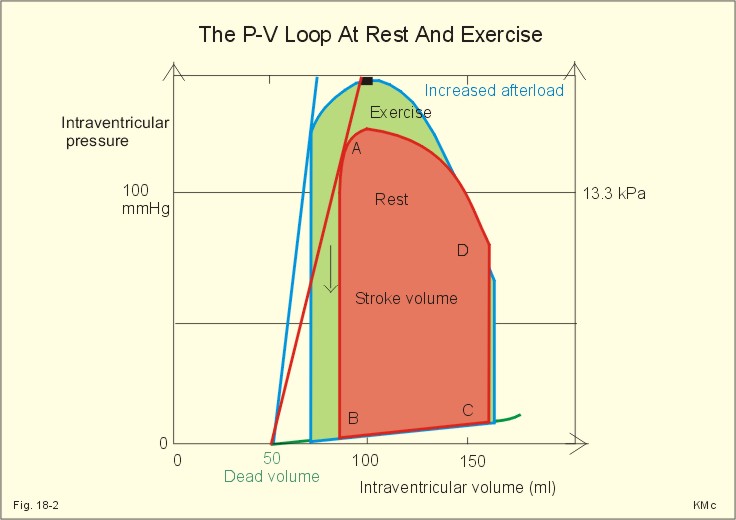
Fig. 18-1: Distribution of cardiac output during exercise. HBF means hepatic bloodflow, and CBF is cerebral bloodflow. A top athlete increases his cardiac output from 5 to 30-40 l of blood per min, when going from rest to maximal dynamic exercise (Fig. 18-1). However, the muscle bloodflow can rise 25 fold in the total muscle mass. Accordingly, the total muscular oxygen uptake rises 85 fold from rest to maximal exercise (see Table 8-1 with calculations). Training improves the capacity for oxygen transport to the muscular mitochondria, and improves their ability to use oxygen. After long-term endurance training the athlete typically has a lower resting heart rate, a greater stroke volume, and a lower TPVR than before. The maximum oxygen uptake progressively increases with long-term training, and the extraction of oxygen from the blood is increased. The lung diffusion capacity for oxygen probably increases by endurance training. The capillary density of skeletal muscles, the number of mitochondria, the activity of their oxidative enzymes, ATPase activity, lipase activity and myoglobin content all increase with endurance training. Endurance training also produces a rise in ventricular diastolic volume. Strength training (weight lifting) produces a rise in left ventricular wall thickness without any important increase in volume During dynamic exercise the stroke volume increases as does heart rate, and the residual ventricular volume decreases (Fig. 18-2).
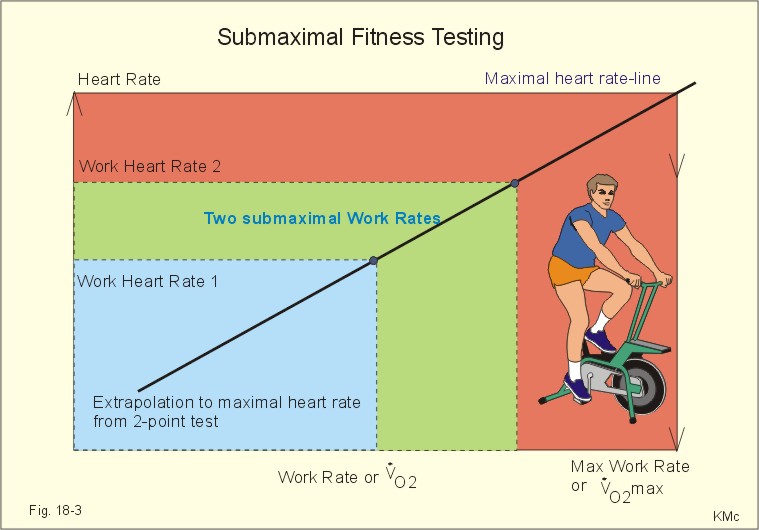
Fig. 18-2: The pressure-volume loop of the left ventricle in a healthy male at rest (red curve) and during dynamic exercise (blue curve). Although the peak ventricular pressure during systole rises considerably and thus the arterial peak pressure, the diastolic pressure falls because of the massive fall in total peripheral vascular resistance. The contractility of the heart is depicted as the slope of the pressure-volume curve. The contractility increases considerably from rest to exercise (Fig. 18-2). A simple objective method of estimating the endurance capacity or fitness number (maximal oxygen uptake, V°O2max) in a person, is to measure the heart rate (HR) at a standardised work on a cycle ergometer. The test rests on the assumption, that there is a linear increase in HR with increasing oxygen uptake or work rate (Fig. 18-3). The net mechanical efficiency is relatively constant in each individual (approximately 20%). On a mixed diet the energy equivalent for oxygen is 20 kJ per l (STPD), so it is easy to calculate the volume of oxygen corresponding to any maximal work rate extrapolated from Fig. 18-3. The test subject wears light clothes, and is not allowed to smoke, eat or work at least three hours before the measurement, which takes place in a comfortable not too warm room.
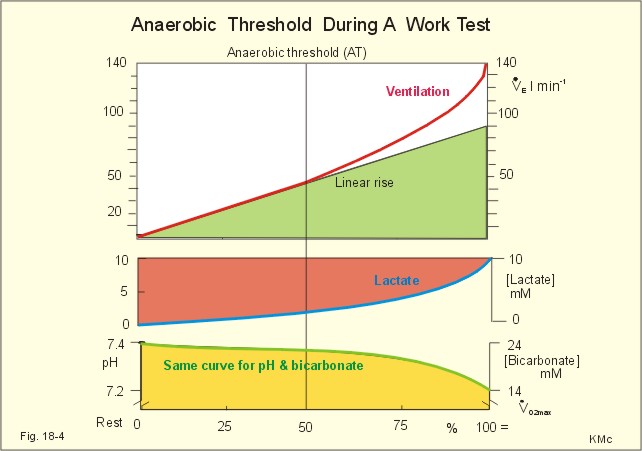
Fig. 18-3: The relationship between work intensity and steady state heart rate at work. The fitness number is in ml STPD oxygen per min and per kg of body weight. The work intensity on the ergometer is chosen to produce a heart rate between 130-150 beats per min, and must be continued for at least 5 min in order to secure respiratory steady state. Respiratory steady state means that the pulmonary oxygen uptake is equal to the oxygen uptake of the tissues. This implies that ventilation and heart rate at work is also stable. As a standard work rate of 100 W is chosen for females, and 150 W is standard for untrained males. An optimally performed fitness test results in a heart frequency of 130-160 beats per min. The submaximal test is designed by P.-O. Åstrand (and is sometimes performed at 2 work rates - Fig. 18-3). Since the rise in HR is linearly correlated to the work rate, a line is drawn through the points (Fig. 18-3). The line is extended until it reaches the horizontal line (maximal HR). Here, the maximal heart rate is the mean of the maximal heart rate of persons of the same age and sex. The rise in mean arterial pressure (MAP) during dynamic exercise is often minimal, because of the arteriolar dilatation with a large, rhythmic bloodflow through the working muscles. The TPVR is typically reduced to 1/4 of the value at rest. In contrast, static exercise often results in a doubling of the MAP, because a large muscle mass is contracting and the contraction is maintained. Static work is typically accomplished with a low cardiac output, so the TPVR is relatively high. This is dangerous to elderly people with known or unknown degrees of atherosclerosis. 3. Limits of exercise performance The limitation of performance (measured as oxygen uptake) depends upon the type of work and upon the person. Several factors are involved. The mass balance principle provides an overview (see Eq. 18-1). Both the maximum cardiac output and the maximum arterio-venous O2 content difference are limiting factors. Healthy persons have redundant ventilation and diffusion capacity in their lungs imposing no limitation. 3.1. Pulmonary ventilation. Increasing work rate (with 15 W more each min) leads to a marked increase in pulmonary ventilation without any ceiling being reached even at maximal oxygen uptake (V°O2max). The steeper rise in ventilation is shown by its deviation relative to the thin line towards the right (Fig. 18-4). Light exercise often increases ventilation by an increased tidal volume (VT). With increasing work rate also the respiratory frequency must rise from 10 towards 50 respiratory cycles per min. The tidal volume can increase to half the value of the vital capacity (6 l), which corresponds to an exercise ventilation of (3*50=) 150 l per min. At exhaustion the ventilation is much greater than at the point, where maximal oxygen uptake is already reached. At this maximum many individuals can increase ventilation further voluntarily. The alveolar gas tensions, PAO2 and PACO2, are essentially maintained during most work rates. At maximal work rate the PAO2 increases and PACO2 decreases 5-10%. This fact illustrates effective gas exchange or adequate ventilation during non-exhausting exercise. Thus ventilation is not the limiting factor in these healthy persons. 3.2. The oxygen utilisation in the tissues is not a likely limitation in healthy people. A group of skiers increased their maximal oxygen uptake further, when they started arm work during continued running. Obviously, the maximal oxygen uptake measured during running is not always maximal. 3.3 Pulmonary diffusion capacity for oxygen with failure of the lungs to fully oxygenate blood. This is certainly not a limiting factor in healthy persons with a redundant lung diffusion capacity. The arterial blood is fully saturated with oxygen even during the most strenuous exercise at sea level. The lung diffusion capacity (DL02) increases, because the number of open lung capillaries is increased, the surface area increases and the barrier-thickness is reduced. In addition, O2 transport is boosted further by the rise in cardiac output from 5 to 30 l of blood per min Oedema or interstitial pulmonary fibrosis leads to thickening of the alveolar-capillary barrier, which will impede O2 exchange. The reason is that the pulmonary vascular volume is reduced (reduced capillary transit time), and thus the diffusion equilibrium point is moved towards the end of the capillary. If patients with lung diseases try to exercise, this problem is further aggravated by the still more reduced capillary transit time. Thus exercise would impose a significant diffusion limitation on O2 transfer. 3.4. Cardiac output. Limited transport capacity for oxygen caused by limited peripheral bloodflow is the only logical explanation. Limitations in reducing TPVR or in the pumping capacity of the heart could cause the limited muscle bloodflow. When work is maintained at peak cardiac output and maximal oxygen uptake, the blood pressure falls as more vasodilatation occurs and there are no signs of even a slight relative increase in the low TPVR. - The major limitation to exercise in well-trained athletes is the heart's pumping capacity in delivering oxygen to the working muscles. The anaerobic threshold (AT) is the exercise level at which the energy requirements can be satisfied only by the combined aerobic metabolism and anaerobic glycolysis. The lactic acid formed in the muscle cells diffuse into the blood and causes a metabolic acidosis, which stimulates the peripheral chemoreceptors. Hereby, ventilation starts to increase out of proportion to the rise in oxygen uptake (Fig. 18-4). Just after the AT is passed, the ventilation increases proportional to the increase in carbon dioxide output (ie, so-called normo-capnic buffering). Accordingly, ventilation increases linearly with carbon dioxide output but out of proportion with the oxygen uptake. The carbon dioxide output and ventilation will increase faster than oxygen uptake, because bicarbonate react with the lactic acid produced, so CO2 is liberated, added to the metabolic CO2 production and eliminated by hyperventilation, causing PaCO2 to fall (ie, hyperventilation) The rise in blood [lactate] is gradual, and Fig. 18-4 does not show any sign of a lactic acid threshold at the anaerobic threshold. Note the total rise in plasma [lactate] of 10 mM, which is equal to the fall in plasma [bicarbonate] from 24 to 14 mM (Fig. 18-4). Exercise levels above the maximal aerobic capacity is called supra-maximal work. Here, the anoxia leading to a metabolic or lactic acidosis contribute with a large ventilatory drive, as shown in the steep component of V°E (Fig. 18-4 and 18-5).
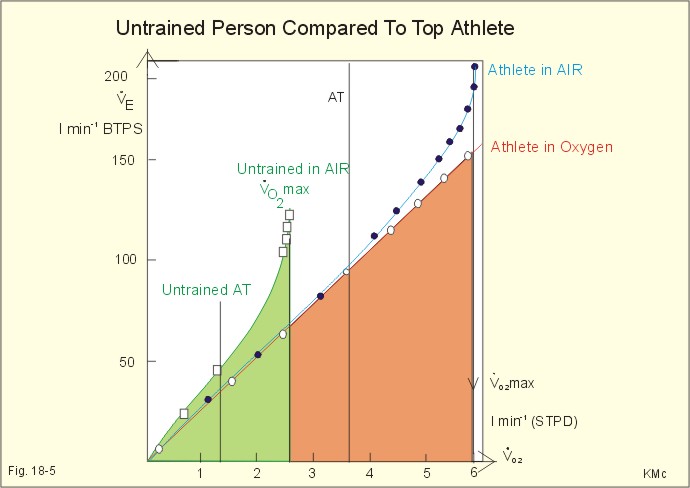
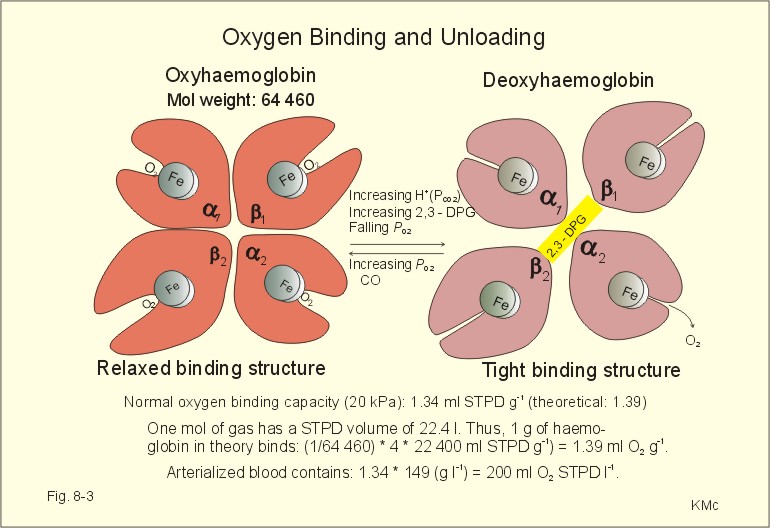
Fig. 18-4: Ventilation and arterial blood concentrations (pH, lactate and bicarbonate) at rest and during an incremental work test on a cycle ergometer up to 100%. Lactate is produced even at light exercise, but only minimal amounts are liberated to the blood (Fig. 18-4). Untrained subjects at any oxygen uptake, have higher ventilation and heart rate than the trained. The AT in untrained persons is often about 50% of maximal oxygen uptake, whereas the AT of athletes approaches 80%. Patients with heart disease increase their blood [lactate] at a minimal activity. The oxyhaemoglobin dissociation curve is moved progressively to the right as exercise intensity increases due to the rise in 2,3-diphosphoglycerate (DPG) concentration (Fig. 8-3) and to the rise in temperature. Above the AT, when oxidative metabolism is high, extra mechanical output is financed by anaerobic energy generation. The end product is lactic acid (Fig. 18-4). The lactic acidosis causes a further shift to the right of the oxyhaemoglobin dissociation curve easing oxygen delivery to the mitochondria. Lactate, nitric oxide and adenosine also dilatate muscle vessels and increase the number of open capillaries, thus improving the diffusion of oxygen from capillary blood to the mitochondria. It is generally believed that the human brain during normal conditions combusts glucose exclusively. This assumption has to be modified. The brain uptake of lactate equals that of glucose during supra-maximal work (Kojiro et al., 2000). 5. Ventilation and oxygen uptake Results from an untrained person with a maximal oxygen uptake of 2.7 l STPD min-1 (AT: 1.3 l STPD min-1), and from a top athlete with 6 l STPD min-1 (AT: 3.6 l STPD min-1) are shown in Fig. 18-5. Several studies have shown oxygen uptake to remain at maximal level despite increasing work rates, and with carbon dioxide output increasing too. These curves also illustrate that ventilation - in these persons -is not the limiting factor for maximal oxygen uptake. If the athlete is suddenly breathing oxygen instead of atmospheric air, while working at a high level (5-6 l STPD min-1), a drastic fall in ventilation will occur within 30 s. This is not a chemoreceptor response, since there is no stimulus. The oxygen breathing reduces the blood [lactate], but not within 30 s. Oxygen breathing abruptly increases the diffusion gradient and thus the rate of diffusion from haemoglobin to the muscle mitochondria. Exhaustive exercise with a severe metabolic acidosis may cause the steep rise in ventilation without a further rise in oxygen uptake (Fig. 18-5). In this case, oxygen seems to diffuse at a reduced rate from haemoglobin to the muscle mitochondria.
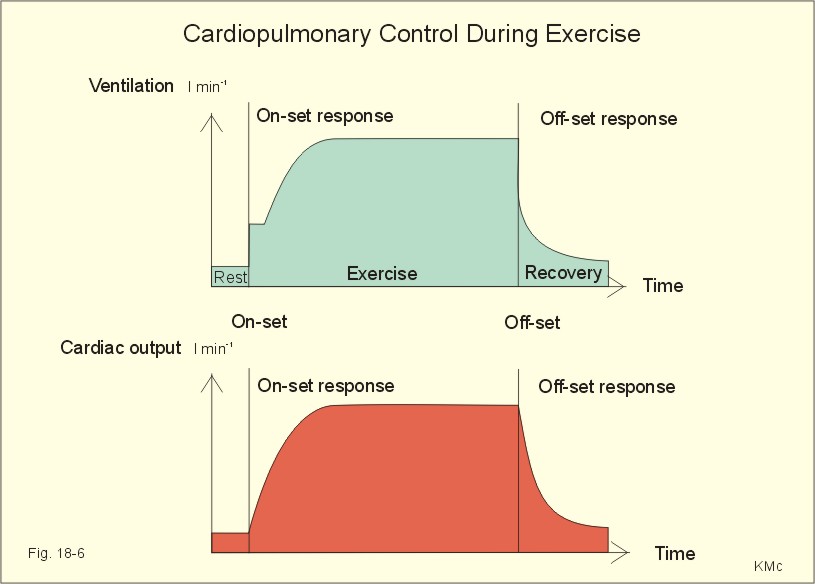
Fig. 18-5: Ventilation and oxygen uptake in an untrained person with a maximum oxygen uptake of 2.7 l per min. Results from a top athlete, with a V°O2max of 6 l min-1 breathing air (•) or oxygen (o) is shown for comparison. Strenuous exercise is also associated with a rise in plasma concentration of catecholamines, dehydration and a rise in core temperature approaching 41o C. The sensitivity of most receptors is increased in an overheated body. Increased activity of the arterial chemoreceptors causes hyperventilation in exercise situations where plasma-K+ is high and PaO2 is dangerously low. The athlete approaches exhaustion and collapse. The proportional increase in ventilation and cardiac output with increasing oxygen uptake suggests a common control system. The integrator consists of sensory and motor cortical areas, and the brain stem neighbour-centres for respiratory and cardiovascular control. The link between the respiratory and the circulatory control system is probably established in the neural network of the brain stem centres. The nucleus of the tractus solitarius is the site of central projection of both chemoreceptors and baroreceptors. The respiratory and the cardiovascular systems are connected during most forms of dynamic exercise (Fig. 18-6), but they can also operate differently. There is a sharp rise in ventilation within the first breath at the on-set of exercise, and cardiac output also increases abruptly (Fig. 18-6). Both variables increase progressively over minutes until a steady state is reached. At the offset of exercise, ventilation and cardiac output falls instantly (Fig. 18-6). The cardiopulmonary adjustments to exercise comprise an integration of I. neural and II. humoral factors. I. The neural factors consist of: 1) Signals from the brain, 2) Reflexes originating in the contracting muscles, and 3) the central & peripheral chemoreceptors. 1. Signals from the brain to the active muscles passes the reticular activating system (RAS) in the reticular formation of the medulla, which includes the respiratory (RC) and cardiovascular centres. This signal transfer is called irradiation from the motor cortex to the RC, and proposed as an explanation of the exercise hyperpnoea. The mesencephalon and hypothalamus are also involved in the Krogh irradiation hypothesis now called central command. Cortical activation of the sympathetic nervous system accelerates the heart, increases myocardial contractility, dilatate the muscular arterioles and contract other vascular beds such as the splancnic region. Speculative mechanisms as irradiation or central command are so-called feedforward hypotheses.
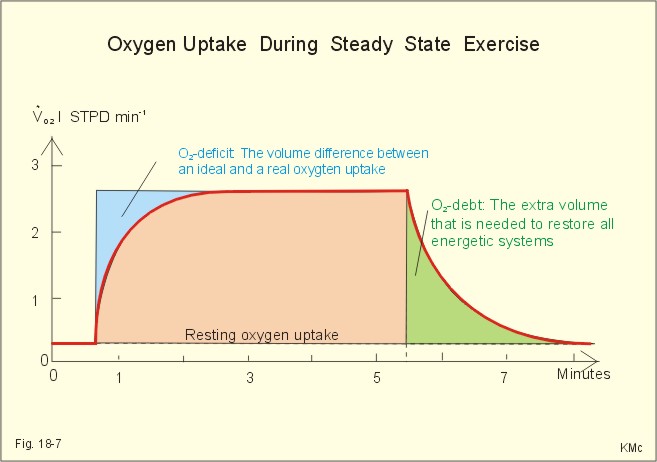
Fig. 18-6: The exercise hyperpnoea and the rise in cardiac output follow the same pattern. 2 Afferent signals from proprioceptors in the active muscles through thin myelinated and unmyelinated fibres in the spinal nerves (type III and small unmyelinated type IV) to RC are the best-documented feedback hypothesis. 3. Central and peripheral chemoreceptors are sensitive to the final product of metabolism, carbon dioxide. The carbon dioxide molecule is most likely the controlled variable, perhaps as PaCO2. The pH, PaO2, and PaCO2 are normal during moderate steady state exercise, where the central chemoreceptors dominate. However, during transitions from rest to exercise and during severe exercise the peripheral chemoreceptors are stimulated. Stimulation of peripheral chemoreceptors increases the rate and depth of respiration and causes vasoconstriction. II. The humoral factors that influence skeletal muscle bloodflow, cardiac output and ventilation are metabolic vasodilatators and hormones. Neural and chemical control mechanisms oppose each other. During muscular activity the local vasodilatators supervene. The local vasodilatators have not been identified. Ischaemic mitochondria in fast oxidative muscle fibres release many vasodilatators such as adenosine, AMP, and ADP. However, it is possible to block many of the neural and humoral factors without disturbing the proportional exercise hyperpnoea and the rise in cardiac output. These experiences suggest that the human body have a redundancy of overlapping control systems. The redundancy-hypothesis, with neural factors dominating at the start of work and peripheral feedback control during steady state, is a logical compromise. The O2 deficit is defined as the difference in O2 volume between an ideal, hypothetical O2 uptake and an actual uptake as it occurs in real life (see Fig. 18-7). The missing O2 volume is the oxygen deficit. The energy demand increases instantaneously at the start of a working period, but the actual O2 uptake via the lung lags behind for 2 min. The oxygen demand deficit is provided for by the O2 stores (oxymyoglobin) and by anaerobic energy.
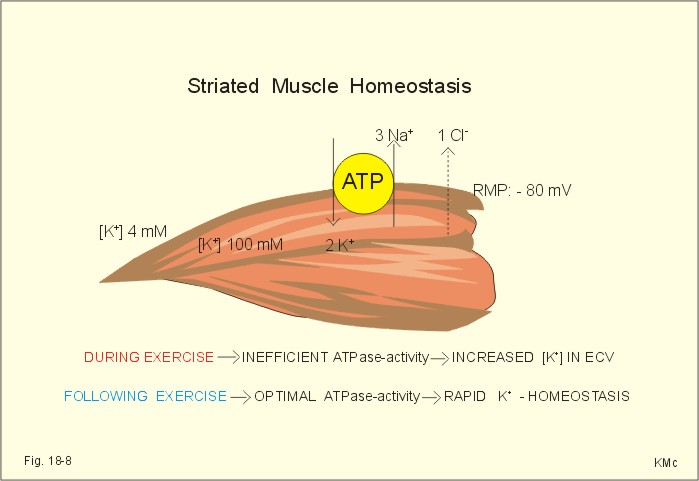
Fig. 18-7: The oxygen deficit and the oxygen debt at exercise. The oxygen debt is defined as the extra volume of O2 that is needed to restore all the energetic systems to their normal state after exercise (Fig. 18-7). The non-lactic O2 debt following moderate work is characterised by maintained blood lactate concentration around the normal resting value of 1 mM. The non-lactic debt is maximally 3 l, used for regeneration of the Phosphocreatine and for refilling the O2 stores. The lactacide O2 debt following supramaximal work (100-400 m dash) can amount to 20 l and the blood [lactate] to as high as 20-30 mM. This O2 debt is used for oxidation of 75% of the lactate produced, and for the formation of 25% of the lactate to glycogen in the liver. Restoration of Phosphocreatine etc following activity, is a process referred to as repayment of the O2 debt. However, it is very uneconomical, since the debt is often twice as high as the O2 deficit. The pathophysiology of sports is related to the ultimate limits of human performance. Severe exercise for prolonged periods, such as a 20-fold rise in metabolic rate in a marathon runner, sometimes result in life-threatening conditions: Histotoxic hypoxia with blockage of ATP production, dehydration, hyperthermia and metabolic acidosis with a pHa below 6.9. Following a short paragraph on 1. Muscle fatigue, two consequences of aggressive attitudes in competitions are dealt with here: 2. Sport injuries and 3. Doping. The final point is 4. Fit for life. Muscular contraction releases a great ionic leak (Na+ -influx and a K+-outflux) through the skeletal muscle membrane, which elicits the action potential (Fig. 18-8). Thus the muscle cell loses K+ and gains Na+ during intensive exercise. Contraction stimulates the Na+-K+-pump acutely, and training increases its activity. Still, at high intensity exercise the ionic leaks can exceed the capacity of the Na+-K+-pump for intracellular restoration. During intensive exercise the Osmolarity of the contracting muscle cells increases together with the capillary hydrostatic pressure. As a consequence, the ECV and plasma volume can fall by 20% within a few min. The plasma [K+] can rise to 8 mM due to efflux from the contracting muscle cells and from red blood cells into a reduced plasma volume. Training reduces exercise-induced hyperkalaemia. Muscle fatigue following prolonged muscle activation increases proportional to the performance and to the loss of muscle glycogen. The insufficient and uncoordinated muscle contractions are due to the lack of glycogen and to failing neuromuscular transmission. Exhaustion of the stores of neurotransmitters in presynaptic terminals can occur within seconds to minutes of repetitive stimulation. Weight lifting, football dash and 100 m dash use up the phosphagen system within seconds. Exhaustion often causes a serious drawback in the systematic practice of an athlete. The body stores are totally depleted, and deleterious consequences may occur.
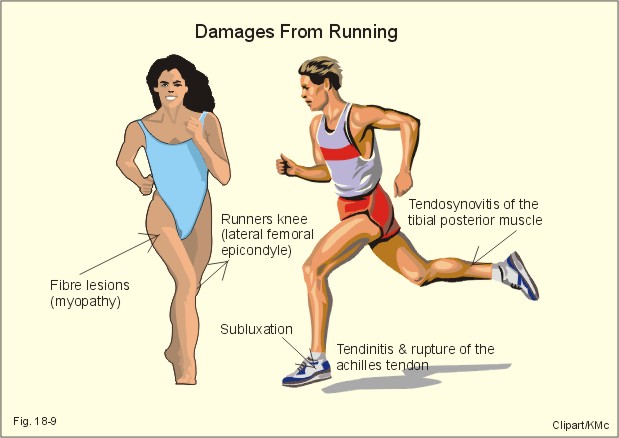
Fig. 18-8: Skeletal muscle cell maintaining homeostasis by the activity of Na+ -K+ -pumps. During exercise the striated muscle cells loose K+ to the ECV and the blood. The Na+ -K+ -pump contains Na+ -K+ -ATPases, which are temporarily inefficient in maintaining homeostasis during exercise (Fig. 18-8). The rise in extracellular K+ is probably related to muscular fatigue and dependent upon the maximal work capacity. Following exercise there is an extremely rapid homeostatic control in healthy well-trained persons. The activity of the Na+ -K+ -ATPases seems optimised in well-trained persons - not necessarily the concentration of Na+ -K+ -ATPases in skeletal muscle biopsies. Even minor diseases, such as a common cold, may reduce cardiac output in an endurance athlete, thus causing muscle ischaemia during the usual practise and extreme muscle fatigue. Isolated muscular fatigue is thus due to depletion of ATP stores, whereby the actin-myosin filaments form a fixed binding and develop rigor or cramps. Neuromuscular fatigue is probably caused by progressive depletion of acetylcholine stores during prolonged, high frequency muscular activity. Fatigue can never be fully explained by a simple rise in plasma-[K+ ] only. Many other signals are integrated in the CNS before a person feels fatigued. Endurance athletics in a hot and humid environment can increase the temperature of the body core to more than 41 oC. Such a level is dangerous to the brain and CNS symptoms and signs develop severe fatigue, headache, dizziness, nausea, confusion, staggering gait, unconsciousness, and profuse sweating. When the victim suddenly faints, this is termed heat stroke, which can be fatal. Five typical categories of sport injuries are considered here. 1. Runners are almost always damaged when working at a too high velocity or high velocity combined with turning or jumping. The force applied to the feet of a 75 kg person while walking is around (Gravity acceleration * body weight) = (9.807 m s-2 * 75 kg) = 750 kg m s-2 or 750 Newton. The force applied to the feet while running is 3-4 fold larger Four typical injuries of runners are shown in Fig. 18-9.
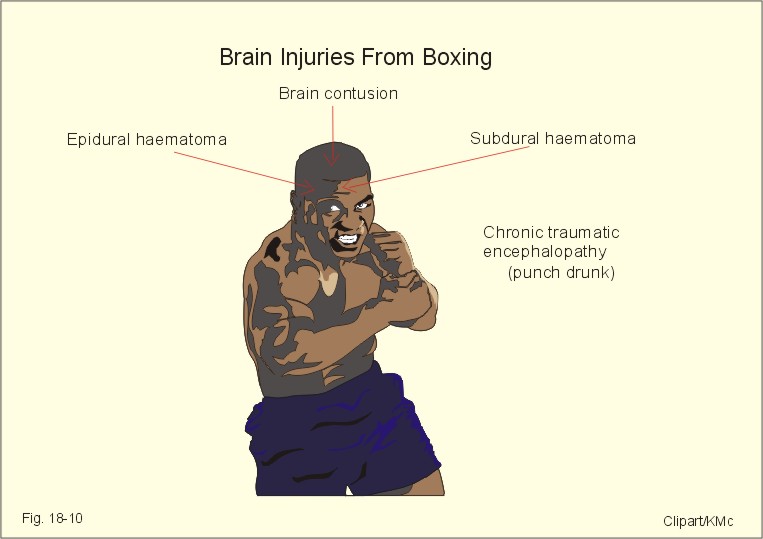
Fig. 18-9:Two athletes showing four frequent leg and foot injuries attended by running. The typical injuries are 1) muscle fibre lesions (myopathy with tender muscles), 2) tendosynovitis (shin splint) of the tibial posterior muscle, 3) tendinitis or rupture of the Achilles tendon, and 4) subluxation of the peroneus muscle tendon. 5) Dome fractures are osteochondral fractures from the talus with pain during running. This often occurs as a complication after a foot distortion, which does not heal. 6) Stress fractures are consequences of walking long distances but are also found after distance running and basketball. These injuries occur during activities (athletes, ball players) with acceleration and deceleration by running or jumping in different directions. Quite often, the athlete is damaged following a break in the training. Even a few days of absence are enough. The athlete starts out too rapidly in order to compensate for the break in the training schedule. 2. Brain injuries (Tableing) are known from serious accidents during many types of sport - in particular Tableing. Even the elegant Tableing legend, Muhammad Ali, was seriously injured during a long - although rather successful - carrier. Acute brain damage or brain contusion includes deeper brain structures with neuronal damage, increased intracranial pressure and brain ischaemia (Fig. 18-10). Head injury during Tableing can result in epidural haematoma (cranial fracture with rupture of the middle meningeal artery). The Tableer hits the floor, is unconscious, wakes up and appears in good condition. Suddenly, he collapses again, and develops hemiplegia or die. The development of subdural haematoma is insidious venous bleeding sometimes with a latency of weeks between the head injury and the clinical phenomena (Chapter 7). CT scanning confirms the diagnosis. In chronic subdural haematoma there is a slow development of headache, drowsiness, confusion, sensory losses, hemiparesis, stupor and coma.
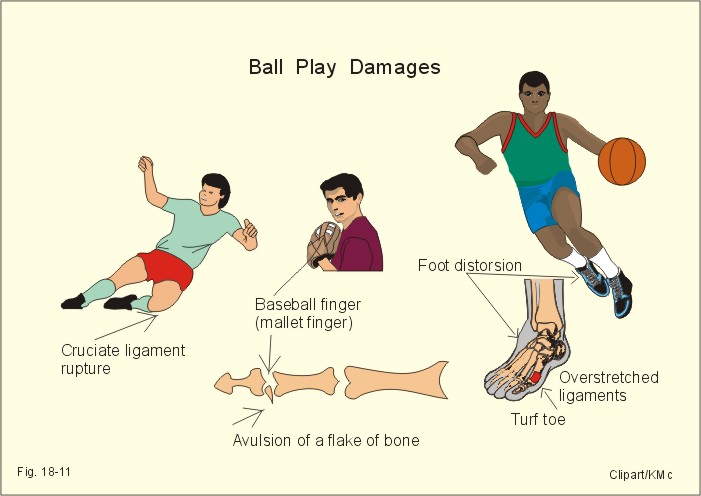
Fig. 18-10: Professional Tableer with typical damages from the carrier. Incomplete recovery from brain damage impairs higher cerebral function, with damages of locomotion (hemiplegia), and of psychological functions (Fig 18-10). The end result for the so-called punch-drunk Tableer is chronic traumatic encephalopathy with dementia, post-traumatic epilepsy and other neurological disorders (Chapter 4). 3.Ball play damages. Cruciate ligament lesions are common from ball play (ie, handball, football, baseball, basket and volleyball). Basketball players often land on the toe tip from height and eventually develop exostoses. The exostosis hallucis is called basketball toe. The nail is tender and the exostosis has to be surgically removed. The tibial anterior muscle originates on the tibia and passes to the navicular bone. Tendinitis in the tendon of this muscle leads to oedema, pain and crepitation.
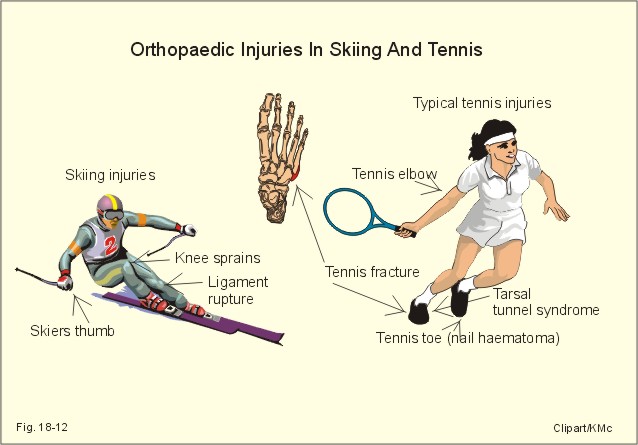
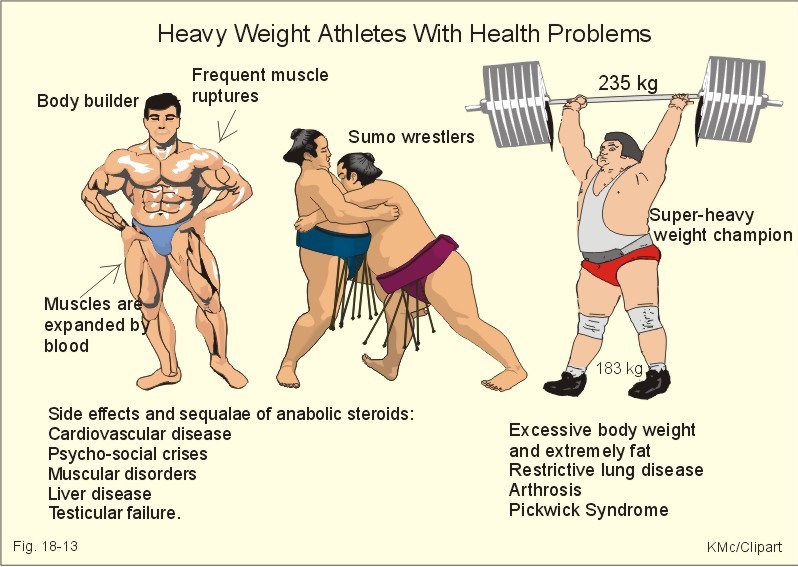
Fig. 18-11: Soccer, baseball and basketball players are shown with typical injuries from the sport. Baseball finger or mallet finger is an avulsion of an extensor tendon of the finger usually including a small flake of bone (Fig. 18-11). Foot distortion (distorsio pedis) frequently includes rupture of the talofibular- calcanofibular- and bifurcate ligament or even fracture (Fig. 18-11). Orthopaedic specialists must handle Malleole and other complicated fractures. Turf toe is overextension of the basal joint of the large toe - frequently during ball play. In this case the large toe is protected with spica plast. 4. Skiing injuries range from trivial to fatal. The incidence of knee sprains is high, because improvements of binding design seem to be unsuccessful. The ski acting as a moment arm (Fig. 18-12) magnifies external rotation of the knee. Slalom skiing is the type of skiing with most fractures. The medial collateral ligament of the knee often ruptures. Fig. 18-12: Typical skiing and tennis injuries are shown in a male and a female. Another common ski injury is the skiers thumb. During a fall the ski pole and the wrist strap tend to concentrate forces to extend the thumb at the mid phalangeal joint until the ligaments burst. 5.Tennis injuries are haematoma subungualis (tennis toe) with bleeding under the nail of the big toe. This is a painful condition - not reserved for tennis players only. The haematoma pressure is relieved by puncture through the nail. The so-called tennis fracture is a fracture of the base of the 5.th metatarsal bone (Fig. 18-12) The tarsal tunnel syndrome is also frequent in tennis players with pains along the medial side of the foot and toes. This involves the tibial posterior nerve in the channel behind the inner Malleole. Tennis elbow is a painful disease of the aponeurotic fibres through which the common extensor origin is attached to the lateral humerus epicondyle. Tennis players from the strain use the name tennis elbow (Fig. 18-12); only few of the sufferers actually play tennis. The demand of fast progress is linked to competitive sports. A better strategy is to practice at a relaxed level, until stamina is developed and hard training is tolerated. Relaxed training is often so comfortable that it becomes a lifestyle. Tender muscles are avoided by prewarming, and a careful muscle stretch program following exercise. Doping derives from the word dope, which means a stimulating drug. Athletes, who use drugs or other means with the intention to improve performance artificially, are doped by definition The list of forbidden drugs counts more than 3500, and it is still growing. Many drugs reputedly increase athletic performance, but the fact remains that such effects rarely show up in double-blind controlled trials. On the contrary, serious side effects occur with a biologically high and statistically significant frequency. Pseudo-doping with Ginseng and a multitude of other extracts and substances is often quite harmless, and - just as many potent drugs - without proven beneficial effect on athletic performance. Anabolic steroidsAnabolic steroids are used to increase muscle strength in females and in male athletes with a poor natural testosterone production - possibly a pure placebo effect. Compared to placebo in double-blind studies there is no detectable steroid-effect on the maximal oxygen uptake, size of the muscles or erythropoiesis. However, both steroids and placebo improves the mood and motivation, so both groups trained more and were eating more than before. As an example, the muscles of body builders are extremely large, but not necessarily equally strong (Fig. 18-13). Some side-effects of dope are lesions of muscle fibres, hypogonadism, liver disorders, and psychosocial deroute (see illustration for further information). The reversible side effects and irreversible sequel are indisputable. Doping addicts have a high risk of cardiovascular diseases (arterial hypertension, atherosclerosis, heart attacks and strokes), muscular disorders, liver disease, and - in males - testicular failure. Both the sperm formation and the testosterone production are suffering, often irreversibly. Body building is considered to be the most doping related discipline - in particular by the use of anabolic steroids - and the results are often monstrous (Fig. 18-13).
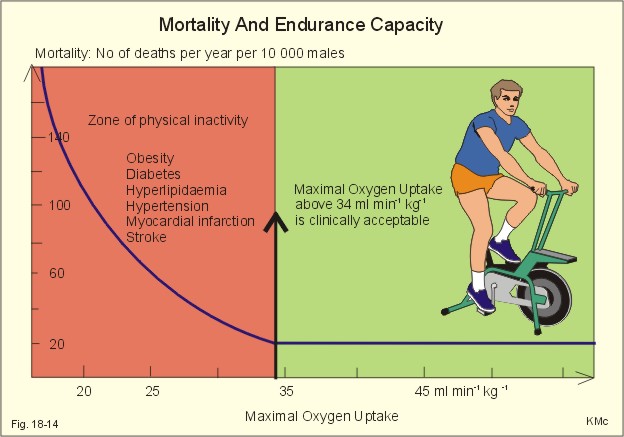
Fig. 18-13: A body builder, a Sumo wrestler and an obese super-heavy weight champion with a world record (235 kg). All have serious health problems. In wrestling, discos and super-heavy weight lifting the use of anabolic steroids is frequently disclosed. A previous world record holder in super-heavy weight lifting developed extreme adiposity when increasing his natural body weight from 80 to 183 kg. The use of steroids resulted in muscular lesions and severe psycho-social crises. The adiposity developed into restrictive lung disease and arthrosis in the knees and other articulations. The athlete was actually a patient with a normal thoracic skeleton, but the lungs were compressed by fat accumulation. During his career he developed the Pickwick syndrome (ie, a fat patient with reduced ventilation, somnolence, sleep apnoea, secondary polycythaemia and cyanosis). The Japanese Sumo wrestlers have the same problems created by the required extreme adiposity, and many excellent wrestlers have obvious difficulties in walking. Blood boosting is an artificial improvement of performance through an increase in the haemoglobin binding capacity. Blood doping (one litre of the athletes own blood) definitely improves the oxygen transport with the blood and also the maximal oxygen uptake, which is beneficial to distance diciplines. Approximately 6 weeks before the competition (Olympic Games or World Championship) the athlete deposits 1000 ml of his own blood as separated red blood cells. The haemoglobin binding capacity is regained by maintained training, and a few hours before the competition, he receives a blood transfusion with his own erythrocytes. Of course, a sudden improvement of the maximum oxygen capacity of more than 10 %, is unfair in endurance disciplines (long distance running, cycling, skiing etc), but it may cause viscosity problems and thrombus formation (see below). High altitude training and erythropoietin High altitude training is a physiological method to obtain the same increase in haemoglobin as in blood doping. The idea is to obtain an advantage not present for most of the other competitors, and thus it is unethical, but impossible to disclose. Training at high altitude implies a larger degree of hypoxia than the same sea level training, so two hypoxic metabolites are produced: Erythropoietin and 2,3-DPG. Erythropoietin increases erythropoiesis and thus the haemoglobin concentration, whereas 2,3-DPG form haemoglobin in the deoxy-conformation and increases the PO2 gradient when delivering oxygen to the muscle cells. A serious development occurred following the introduction of industrially produced human erythropoietin (EPO). Natural production is increased, if there is hypoxia in the kidneys. Erythropoietin is clearly beneficial to endurance athletes, but most types of doping have deleterious effects. The synthesised erythropoietin, when administered to athletes, definitely stimulates the red bone marrow to increase the production of erythrocytes. The effect on the maximum oxygen capacity is indisputable, but the price is often death, because of fluid loss, Haemo-concentration, drastically increased blood viscosity and thrombus formation all over the circulatory system. The death of a whole group of young racing bicyclists, within a short period of time, was probably caused by erythropoietin. Ephedrine, amphetamine and other psychomotor CNS stimulants are still used by athletes in the hope of increased velocity (so-called speed). Amphetamine or speed pills have improved results in running, bicycling, swimming, weight-throwing and other disciplines compared to placebo. The same stimulants have increased blood pressure and heart rate in athletes exercising heavily in hot climates, until they died from cerebral bleeding or ventricular fibrillation. This has taken place several times in the history of Tour de France. Cocaine and coffeine seem to suppress natural fatigue, and is also on the doping list. Suppression of natural fatigue leads to exhaustion and circulatory collapse sometimes with cerebral bleeding and ventricular fibrillation. b-Adrenergic blockers are drugs that reduce heart rate (negative chronotropic effect) and the force of contraction (negative inotropic effect). Both mechanisms reduce the myocardial oxygen demand. In precision sports, where relaxation without tremor is essential, these drugs have a proven beneficial effect in double-blind controlled clinical trials, and they are therefore on the doping list. Precision sports include archery, standard pistol, skeet shooting, rifle shooting, ski jumping, billiards, etc. Participation is ski-shooting competition is hardly advantageous on b-blockers, because the abuser gets too tired to accomplish endurance performance. The athletes in disciplines with specific weight classes - such as Tableing, wrestling, weight lifting etc - reputedly use diuretics in order to cause a rapid weight loss, with the advantage of competing against smaller persons. Uncontrolled use disturbs the normal distribution of ions in the cells and body fluids, and reduces the blood volume and increases viscosity. In extreme cases there is circulatory collapse and death. Gonadotropins - in particular the luteotropic hormone (LH) - stimulate release of testosterone from the Leydig interstitial cells of the testes. Human chorion Gonadotropin (hCG) also binds to the Leydig cells and releases testosterone in males. Corticotropin (ACTH) from corticotropic cells of the adenohypophysis stimulates production and secretion of adrenal cortical hormones (mainly glucocorticoids). Somatotropin (human growth hormone, HGH) from somatotropic cells of the adenohypophysis increases and regulates growth, partly directly and partly through evoking the release of somatomedins from the liver. HGH increases protein synthesis, lipolysis and blood glucose. HGH induces gigantism in growing individuals and acromegaly in adults. Uncontrolled use may lead to cardiomyopathy, diabetes, adiposity, articular pain, hypertension and early death. Monstrous growth of the shoulders and bodies of female swimmers is disclosed by vision alone, and the sight is clearly different from a naturally top- trained female. Some of the female track runners have written history by winning WM and the Olympics for females year after year, although they looked like a male. Pregnancy seems to increase muscle strength in female athletes. Female top athletes - just following the period, where they gave birth to their first child - have set several world records. Of course, this is acceptable as a natural and unintended event. However, in some countries female athletes have become pregnant for 2-3 months, in order to improve their performance just following an abortion. Genetic doping In countries where the political will, is not balanced by ethics, recombinant DNA technique may be used in the future to clone groups of individuals with remarkable talents for special athletic performances. Smoking has acute and deleterious effects on both the cardiovascular and the respiratory system, but athletes have used it. The substances involved are not at the doping list. The CO blocks off part of the haemoglobin, and limits the transport capacity for oxygen to all mitochondria, which is especially inhibitory to the heart and the skeletal muscles. Nicotine constricts terminal bronchioli and arterioles in many vascular beds. Nicotine also paralyses the cilia of the epithelial cells of the respiratory tract. Chronic smoking leads to life-long chronic bronchitis and emphysema or to lung cancer. A high endurance capacity or fitness is healthy. The mortality increases with low endurance capacity in males (Fig. 18-14). A similar pattern is recorded for females. An endurance capacity (fitness number, V°O2max) of 34 ml O2 min-1 kg-1 or more seem compatible with a reasonable health status and mortality risk.
Fig. 18-14: The endurance capacity (V°O2max) in relation to mortality. The total mortality is given as Number of deaths per year per 10 000 males. Physical inactivity with an endurance capacity (fitness number) below 34 ml min-1 kg-1 is a risk factor for the development of atherosclerosis, other risk factors and sudden death in males - and probably also in postmenopausal females. · The principle of mass balance states that cardiac output is equal to the oxygen uptake (V°O2 ) divided by the arteriovenous oxygen content difference:
· The following is valid for exercising healthy males (up to 70% of their maximal oxygen capacity, V°O2max): Eq. 18-2: Q° litre min-1 = 3.07 + 6.01 × V°O2 . · This calculation of Q° allows for estimation of the rarely available mixed venous carbon dioxide concentration (Cv¯CO2 ) from Fick's principle:
· The diffusion-limited oxygen uptake ( V°O2 ) equals the product of lung diffusion capacity (DL02 ) and the mean alveolar oxygen tension gradient (DPO2):
· Poiseuilles law relates bloodflow (Q° ) to total peripheral vascular resistance (TPVR) and the mean arterial driving pressure (MAP):
The following five statements have True/False options: A. Fatigue can never be fully explained by a simple rise in plasma-[K+ ] only. B. Fitness tests rest on the assumption, that there is an exponential increase in HR with increasing oxygen uptake or work rate. C. Erythropoietin clearly improves the endurance capacity of athletes. D. Erythropoietin is produced and secreted from the kidneys. E. At maximal works the lung diffusion capacity for oxygen rises to 9 ml STPD s-1 kPa-1 . A 32-year old marathon runner (body weight 60 kg) is examined on a treadmill. He is running at a velocity of 16 km per hour. The following variables are measured: Q°= 25 l per min, CaO2 = 200 and Cv¯O2 = 40 ml (STPD) per l of blood. The concentration of lactic acid is measured in the blood every second min for 18 minutes. The level increases from 1.1 to a steady state value of 15 mM. The total work rate of the heart (pressure-volume work and kinetic work) is 16 Watts or 16 J per second, and the mechanical efficiency of the heart work is assumed to be 20%. The energy equivalent for oxygen on a mixed diet is 20 kJ per l (STPD) of oxygen. 1. Calculate the oxygen uptake of the heart during this work. 2. Assume that the arterio-venous oxygen content difference for the heart is equal to that of the whole body. Calculate the coronary bloodflow during running. 3. Has the athlete accumulated an important oxygen debt during the 18 minutes of running? A male world record holder in 100-m dash is examined on a treadmill with a velocity capacity up to 35 km per hour. His body weight is 78 kg. While standing relaxed on the treadmill before exercise, his oxygen uptake is measured to 300 ml STPD min-1. The ventilatory exchange quotient (R ) in respiratory steady state, is measured to 1.0. At a given signal the athlete jumps on the running treadmill and performs a 20-second dash similar to a 200 m dash on the track. The inspired, atmospheric air has an oxygen fraction (FIO2) of 0.2093 and a carbon dioxide fraction (FICO2) of 0.0003. As soon as he jumps off the treadmill, he is connected to a system of rubber bags, where his expired air is collected over the next hour until his resting oxygen uptake is re-established. All the expired air in the rubber bags is mixed and analysed. The mixed expired air fractions are FEO2 = 0.1746 and FICO2 = 0.035. The volume of mixed expired air is measured at ATPS, and by calculation corrected to a STPD volume of 1090 litres. 1. Calculate the oxygen debt repaid over the 1-hour post-exercise period. 2. What assumptions is maid in order to perform this calculation? 3. Calculate the ventilatory exchange quotient in the post-exercise period and compare the result to the pre-exercise R-value. 4. What is the basis of oxygen debt? A well-trained male long distance skier, weight 74 kg, has a V°O2max of 6 l STPD min-1 .The maximal arterio-venous oxygen content difference is 150 ml STPD l-1 of blood. During maximal work his lung diffusion capacity for oxygen (DLO2) rises to 9 ml STPD s-1 kPa-1. 1. Calculate maximum cardiac output and describe the consequences for the lung perfusion. 2. Calculate the fitness number and explain what it means. 3. Define the mean oxygen tension gradient for lung diffusion and calculate its size. Explain how the gradient can increase to this extent. A female 20 years of age, with a body weight of 62 kg, is exercising on a bicycle ergometer during steady state. Her cardiac output (Q°) is measured to 25 l min-1 by the mass balance principle with carbon dioxide as indicator, and her arteriovenous O2 content difference is measured to 170 ml STPD l-1. 1. Calculate her oxygen-uptake per min (V°O2). 2. What assumption must be made in order to calculate her fitness? An adult male has a lung diffusion capacity for oxygen of 22 ml STPD per min and per mmHg, and a mean alveolar O2 tension gradient of 12 mmHg. His oxygen concentration in the arterial blood (CaO2) is 200 ml per l and the renal bloodflow (RBF) is 1200 ml per min. The renal O2 consumption is 15 ml per min. 1. Calculate his oxygen uptake in ml STPD per min. 2. How is it possible for this person to increase the oxygen uptake to 4900 ml STPD per min? 3. Calculate the arteriovenous oxygen content difference in the kidneys. 4. Is the oxygen delivery to the kidneys redundant? Try to solve the problems before looking up the answers. · The total muscular oxygen uptake can rise by a factor of 80 from rest to maximal exercise. · At the start of exercise, signals from the brain and from the working muscles bombard the cardiopulmonary control centres in the brainstem. Both cardiac output and ventilation increase, the a-adrenergic tone of the muscular arterioles falls abruptly, whereas the vascular resistance increases in inactive tissues. · The circumventricular organs of the brain contain many fenestrations, and they are located close to the control centres of the hypothalamus and the brainstem. · Training improves the capacity for oxygen transport to the muscular mitochondria, and improves their ability to use oxygen. After long-term endurance training the athlete typically has a lower resting heart rate, a greater stroke volume, and a lower peripheral resistance than before. · The V°O2max progressively increases by endurance training, and also the extraction of oxygen from the blood increases. · At maximal work the lung diffusion capacity for oxygen (DLO2) rises to 9 ml STPD s-1 kPa-1 (from 3.6 at rest). The lung diffusion capacity for oxygen increases by endurance training. · According to the redundancy hypothesis, the rise in cardiac output and in ventilation during exercise is caused by an integration of neural and humoral factors. · The demand of fast progress is linked to competitive sports. A better strategy is to practice at a relaxed level, until stamina is developed and hard training is tolerated. · Relaxed training is often so comfortable that it becomes a lifestyle. Tender muscles are avoided by prewarming, and a careful muscle stretch program following exercise. · Amphetamine or speed pills and other CNS stimulants have improved results in running, bicycling, swimming, weight-throwing and other disciplines compared to placebo. The same stimulants have increased blood pressure and heart rate in athletes exercising heavily in hot climates, until they died from cerebral bleeding or ventricular fibrillation. · Pregnancy/Abortion as doping. Pregnancy seems to increase muscle strength in female athletes. Female top athletes have set world records, just following the period, where they gave birth to their first child. - In some countries female athletes have become pregnant for 2-3 months, in order to improve their performance just following an abortion. · Blood doping definitely improves the oxygen transport with the blood and also the maximal oxygen uptake. · Doping with erythropoietin stimulates the red bone marrow to increase the production of erythrocytes. The beneficial effect on the maximum oxygen uptake is indisputable, but the prize has been death because of thrombus formation. · Doping addicts have a high risk of cardiovascular diseases (arterial hypertension, atherosclerosis, heart attacks and strokes), muscular disorders, liver disease, and - in males - testicular insufficiency. Both the sperm formation and the testosterone production are suffering, often irreversibly. · Lack of fitness is a risk factor for the development of atherosclerosis and for sudden death. Medicine and Science in Sports and Exercise. Monthly journal published by the Am. College of Sports Medicine. Williams & Wilkins Co, 428 East Preston Street, Baltimore MD 21202-3993, USA. Apps DK, Cohen BB and CM Steel. Biochemistry. Bailliere Tindall, London, 1994. Katzung BG. Basic & Clinical Pharmacology. 11th Ed. Appleton & Lange, Stanford, Connecticut, 2007. Kojiro et al. J.Physiol. (London) 522. 1, 159-164, 2000. Wood, S C, and R C Boach: Sports and Exercise Medicine. Marcel Dekker Inc, N.Y. 1994.
|
||
.jpg){kind=link}
{kind=link}
Click here to introduce your comments or contributions