New Human Physiology | Paulev-Zubieta 2nd Edition
Chapter 6:The Autonomic Nervous System and Disorders
| HOME | PREFACE | TABLE OF CONTENTS | SYMBOLS | SECTION INFO | CONTRIBUTORS | LINKS | CONTACT US |
Highlights
Study_ObjectivesPrinciplesDefinitionsEssentials
PathophysiologyEquationsSelf-AssessmentAnswers
Further Reading
|
|
|
 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
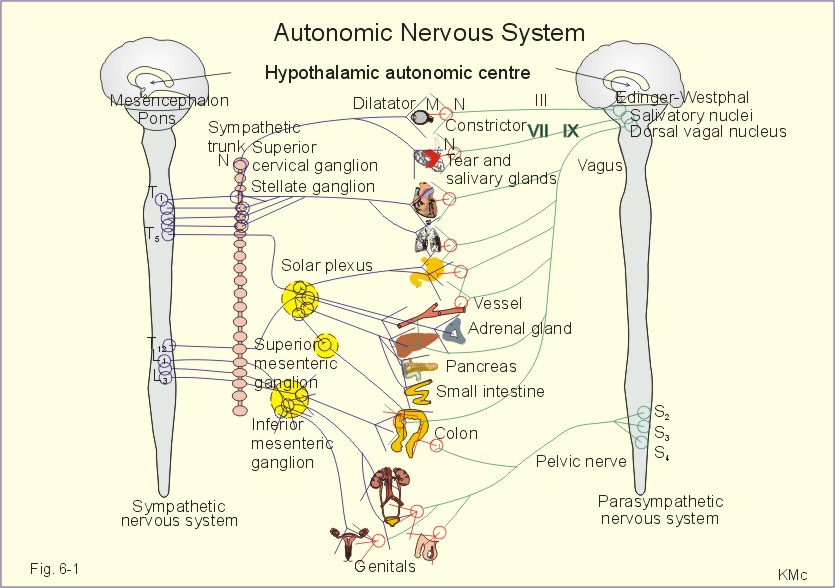
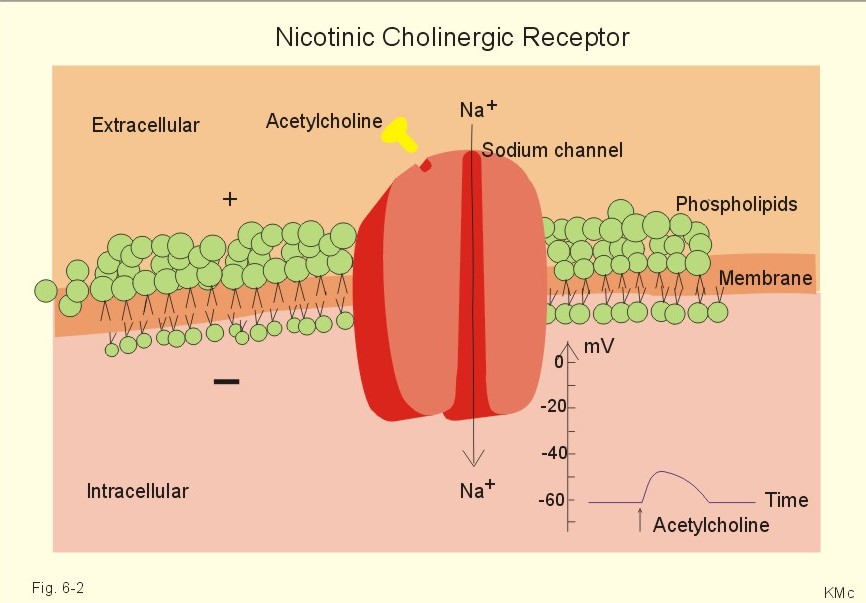
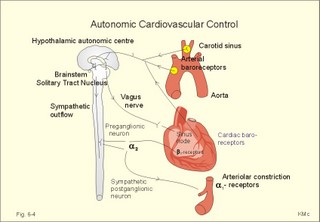
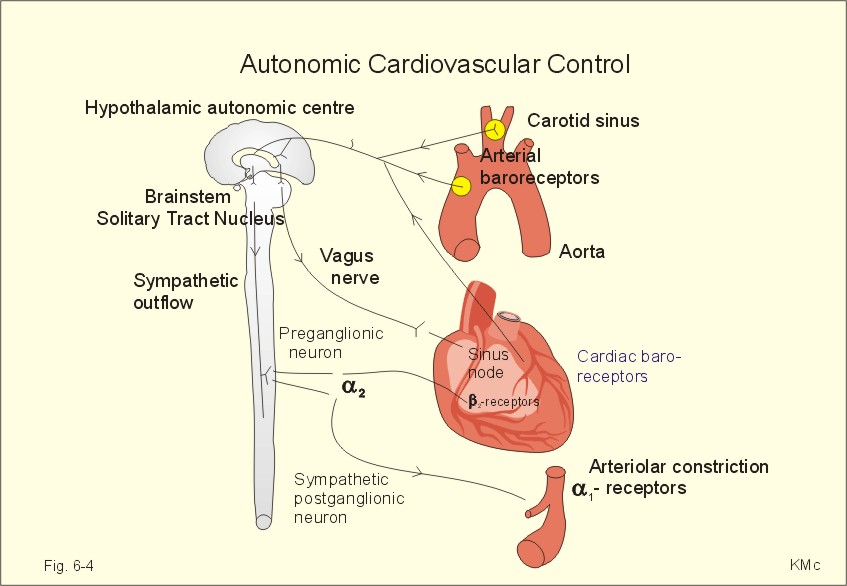
This paragraph deals with 1. The autonomic system in general, 2. The sympathetic system, and 3. The parasympathetic system. 1. The Autonomic System In General The autonomic system directly influences smooth muscles, glands and the heart through its two subdivisions, the sympathetic and the parasympathetic system. The two subdivisions function in a dynamic balance aiming at homeostasis.The enteric nervous system is lying within the walls of the gastrointestinal tract and includes neurons in the pancreas, liver and gallbladder, thus being an entity in itself. However, the enteric nervous system is clearly an important part of the autonomic nervous system that controls gastrointestinal motility, secretion and bloodflow.The central autonomic systemThe central autonomic nervous system outflow arises in the hypothalamus, the brainstem, and the spinal cord. The motor and premotor cortex, the cingulate gyrus and the hypothalamus can modulate the function of the autonomic medullary control neurons in the lateral horn of the grey matter. Circulatory changes during exercise and in various stressful situations are influenced or governed by the cortex and deeper brain nuclei. The central autonomic system also modulates release of certain peptides and catecholamines that affect both blood volume as well as the total peripheral vascular resistance.The cerebral cortex assimilates all inputs of visual, olfactory, labyrinthine, locomotor origin, as well as from other specialised sensors (stretch receptors, chemo-, baro-, osmo-, and thermo-receptors).The integration of these inputs into an appropriate response takes place in the hypothalamus and in the ponto-medullary centres. From here the efferent signals pass to the periphery via the sympathetic and the parasympathetic pathways.The primary afferent projections from the baroreceptors reach the solitary tract nucleus (STN), and from here we have connections to the important dorsal motor nucleus of the vagus (DMNV in Fig. 6-4). A high baroreceptor activity stimulates the DMNV, so that the vagal inhibition of the heart is increased. More importantly, the high baroreceptor activity inhibits the sympathetic drive to the heart and vessels thus reducing blood pressure (Fig. 6-4).The central autonomic structures co-operate in situations of survival character: Fright, flight or fight- response, feeding and drinking in starvation, reproduction and sexual satisfaction for continuation of life, thermoregulation at extreme temperatures and emotional behaviour in crises. The Fright -Flight Or Fight Response Aggression and defence responses are elicited in emergency situations. The sympatho-adrenergic system gives rise to the fright, flight or fight-reactions in acutely stressful situations. The sympathetic reactions dominate over the parasympathetic and the subject is aggressive or anxious. The brain releases corticotrophin-releasing factor to the hypothalamic-pituitary portal system. The hypothalamic-pituitary axis secretes adenocorticotropic hormone, the cardiac rate and contractile force increases, the blood is distributed from viscera to the active skeletal muscles by visceral vasoconstriction and preferential vasodilatation. The subject hyperventilates, the gastrointestinal activity is reduced, and there is increased glycogenolysis and lipolysis. The airways dilatate, and the adrenal medullary (catecholamines) and cortical secretion (cortisol) increases. This response is seen in humans exposed to psychological-emotional stress. Stress in general is comprised of severe emotional and physical burdens (fear, pain, hypoxia, hypothermia, hypoglycaemia, hypotension etc).Cannons emergency reaction is an immediate sympatho-adrenergic response to life-threatening situations, with both sympatho-adrenergic and parasympathetic overactivity. The last phenomenon includes vagal cardiac arrest with involuntary defecation and urination.Feeding and drinkingBilateral destruction of the ventromedial hypothalamic nuclei leads to hyperphagia and failure of body weight control. Such animals become obese, and they have high plasma [insulin].Bilateral lesions in the lateral hypothalamic regions cause a temporary hypophagia.The cells of the ventromedial nuclei have a special affinity for glucose, and these cells are responsible for insulin secretion from the pancreatic b-cells. Signals from the dorsal motor nucleus of the vagal nerve increase insulin secretion, and sympathetic stimulation inhibits the release of insulin. The ventromedial nuclei seem to function like a glucostat.Stimulation and ablations of the limbic system affect food intake. Obviously from clinical practice, psychological factors, emotional disturbances, motivations and conditioned behaviour are all affecting our drive for food intake.Concerning the control of food intake see also Chapter 20 and 27.Sexual behaviourHypothalamic and other limbic system co-operation are responsible for a wide variety of autonomic and somatic phenomena associated with emotions. Stimulation of the midbrain septum yields pleasurable sensations and sexual drive in patients. The dorsomedial nucleus of the hypothalamus is probably a major sex centre responsible for the sexual act. Stimulation of the ventromedial and preoptic regions also releases sexual activities. See also Chapter 29. Thermoreceptors can initiate generalised reactions to heat and cold. The signals from both superficial and deep thermoreceptors must act through the hypothalamus to arouse appropriate, generalised reactions.Cooling or heating the denervated lower extremities of spinal men evoked vasoconstriction and shivering or vasodilatation and sweating of the innervated upper body shortly after cooled or warmed arterial blood reached the brain. The anterior hypothalamus is responsible for sensing blood temperature variations. The anterior hypothalamus, in particular the preoptic area, has been shown to contain numerous heat-sensitive cells and less cold-sensitive receptors. Such central thermoreceptors are also found at other levels of the CNS. After destruction of the hypothalamus, the midbrain reticular formation takes over the temperature control. Sections eliminating both the hypothalamus and the mesencephalon leave the medulla and spinal cord to control temperature. The posterior hypothalamus does not contain thermoreceptors. Concerning thermocontrol see also Chapter 21.The brain and the immune defence systemInternal and external stress affects the prefrontal cortex, whereby the limbic system with the hypothalamus is activated. Hypothalamic nuclei release corticotropin-releasing hormone (CRH) to the portal blood. The blood reaches the adenohypophysis, where CRH triggers the release of adenocorticotropic hormone (ACTH), endorphins and met-enkephalin. ACTH works through different pathways in order to protect the body. ACTH stimulates the adrenal cortex to release corticosteroids, which produce immuno-suppression. Immuno-suppression reduces the number of inflammatory effector cells, including helper T cells and killer cells.On the other hand, cancer therapists assume that relaxed lifestyle and positive reinforcement may have stimulated the immune defence in some patients with malignant diseases, and explain miraculous remissions. Higher brain centres may even affect the reticuloendothelial production of killer cells through the peripheral nerves to the lymph nodes and bone marrow. See also Chapter 32 . Fig. 6-1: The peripheral autonomic nervous system. b -receptors stimulate glycogenolysis in the liver and lipolysis in lipid tissues. Autonomic nerves are composed of two neurons termed the preganglionic and the Postganglionic neuron based on anatomical location relative to the ganglion. A preganglionic neuron has its cell body in the spinal cord or brainstem and is modulated by higher centres and by spinal reflexes (Fig. 6-1). The preganglionic axon leaves the CNS from the cranial, thoracic, lumbar or sacral regions and synapse in the autonomic ganglia with the cell body of the postganglionic neuron. The postganglionic neurons innervate the effector organs (Viscera).Viscera function involuntarily and their activity must be modulated by the autonomic nervous system with excitatory or inhibitory signals. All autonomic nerves have ganglia outside the CNS in contrast to the somatic nervous system, where neural connections are located entirely within the CNS. Most somatic nerves that control motor function are myelinated and have a high conduction velocity, whereas most postganglionic neurons are unmyelinated with a low conduction velocity. However, the preganglionic neurons are mostly myelinated with a high conduction velocity (Fig. 6-1). Receptors for neurotransmitters are specific cellular components, whose interaction with the neurotransmitter, a hormone or a drug produces a biological response in the cell. Acetylcholine (ACh) is the transmitter between the pre- and the post-ganglionic neurons, not only in the sympathetic nervous system, but also in the parasympathetic system. The cholinergic receptors are nicotinic or muscarinic. The cholinergic receptors of the ganglia and in the somatic motor endplate are nicotinic. Nicotine and acetylcholine activate nicotinic cholinergic receptors. When the action potential arrives at the preganglionic fibre, acetylcholine is released from its terminals and diffuses across the synaptic cleft to bind to the specific nicotinic receptors on the membrane of the postganglionic neuron. Nicotinic receptors are linked to cation channels lined with negative charges. These channels open enough to allow mainly hydrated Na+ to enter the cell rapidly (for about 1 ms) and depolarise the membrane (Fig. 6-2).
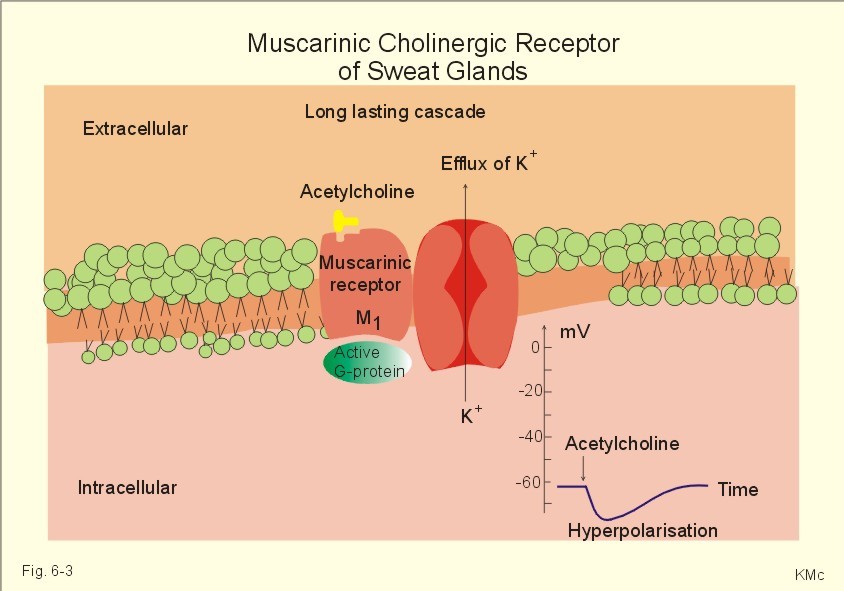
Fig. 6-2: The nicotinic cholinergic receptorThe resulting current elicits an excitatory postsynaptic potential (EPSP). Repolarisation is also fast (ms).Acetylcholine is also the neurotransmitter for the sympathetic innervation of sweat glands, and they are completely blocked by atropine. The acetylcholine receptors of the sweat glands are muscarinic, since acetylcholine and muscarine (Fig. 6-3) activate them.
Fig. 6-3: The muscarinic cholinergic receptorThese slowly working surface-receptors are linked to a long lasting cascade of events starting with binding of the hormone to the receptor, activation of G-proteins (see Chapter 7), enzyme activation, production of second-messengers, protein kinase activation, and phosphorylation of specific proteins such as channels. All these processes are simplified in Fig. 6-4, and the result is opening of K+-channels, with efflux of K+, so the membrane is hyperpolarised. In this example, acetylcholine is an inhibitory transmitter. 2. The Sympathetic Nervous System The preganglionic sympathetic nerve fibres originate in small multipolar neurons in the lateral horn of the grey matter in the thoracic and lumbar spinal cord. The central sympathetic outflow converges on these preganglionic neurons. Their axons are thin myelinated fibres that leave the spinal cord through the ventral root. The preganglionic fibres then leave the spinal nerve forming myelinated white rami communicantes, through which they reach the nearest ganglion in the paravertebral ganglia of the paired sympathetic trunk. Typically, each fibre will end here forming synapses with up to 20 postganglionic neurons. A few preganglionic fibres pass the sympathetic trunk without interruption to form the splancnic nerves that reach the three unpaired prevertebral ganglia (coeliac = solar plexus, superior mesenteric and inferior mesenteric) of the lower intestinal and urinary organs. Most sympathetic ganglia are remote from the organ supplied. The postganglionic fibres are all unmyelinated, and they leave the sympathetic trunk through the grey rami communicantes and thus reach the effectors supplied by the sympathetic system. The effectors are the smooth muscles of all organs (blood vessels, viscera, lungs, hairs, pupils), the heart and glands (sweat glands, salivary and other digestive glands). In addition, the sympathetic postganglionic fibres innervate adipocytes, hepatocytes and renal tubular cells.The sympatho-adrenergic system is a functional and phylogenetic unit of the sympathetic system and the adrenal medulla. The adrenal medulla is a modified sympathetic ganglion. Any increase in sympathetic activity increase the secretion of adrenaline and noradrenaline from the medulla into the circulation. The preganglionic fibres to the adrenal medulla pass all the way to the special postganglionic cells in the adrenal medulla. The synapse is cholinergic (nicotinic) as it is for all preganglionic synapses. The postganglionic cells of the adrenal medulla have developed to cells filled with chromaffine granules, and are called chromaffine cells. These cells do not conduct signals, but synthesise adrenaline (and noradrenaline) which is released into the blood. Sympathetic stimulation triggers the conversion of tyrosine to dihydroxyphenylalanine (DOPA). A non-specific decarTableylase catalyses the conversion of DOPA to dopamine, which is taken up by the chromaffine granules in the cells. The granules contain the crucial enzyme, dopamine b-hydroxylase. This enzyme is activated by sympathetic stimulation, and catalyses the formation of noradrenaline from dopamine.A few granules store noradrenaline (NA), while the remaining granules liberate NA to the cytosol, where NA is methylated by phenylethanolamine N-methyltransferase to adrenaline. Adrenaline is taken up by chromaffine granules and stored as the predominant adrenal hormone. The sympathetic system exerts either excitatory or inhibitory actions through adrenergic receptors. Adrenergic receptors are membrane-receptors. The dual response to adrenergic stimulation was known before Ahlquist in 1948 proposed that adrenergic receptors could be divided into two groups, a- and b- receptors, on the basis of blocking drugs (Table 6-1). The basic idea of Ahlquist is that noradrenaline (NA) act predominantly on vasoconstricting a-receptors, and isoprenaline (Iso) predominantly on vasodilatating b-receptors. Both types of receptors are stimulated by adrenaline (Ad).
The near-vision response is also called the convergence response. Near vision -even with only one eye - triggers accommodation and pupillary contraction (Table 6-1). The ciliary muscle and the pupillary sphincter muscle are innervated of the parasympathetic oculomotor nerve, and the two muscles (with M-receptors) contract simultaneously for near vision. This leads to increased refractive power or accommodation, and to pupillary contraction (miosis).When a person closes his eyelids the pupils enlarge, and when he opens the pupils again the pupils become smaller. This is due to the pupillary light reflex, where retinal ganglion cells are stimulated by light, send signals through the optic nerve to the olivary pretectal nucleus neurons. These light-sensitive neurons are connected to the parasympathetic preganglionic neurons in the oculomotor Edinger-Westphal nuclei on both sides. The light reflex contracts the pupillary sphincter muscle. Argyll-Robertson’s pupillary syndrome refers to small, light-refractive pupils with maintained convergence response to near vision. The syndrome is seen in neurosyphilis, when the pupillary light reflex is spoiled by interruption of the fibres from brachium to the olivary pretectal nucleus neurons.Sympathetic preganglionic neurons in the intermediolateral cell column of segment T1-T2, send ascending axons to the superior cervical ganglion. Postganglionic axons follow the ciliary nerve into the eye. The nerve terminals end on a 1- receptors on the dilatator pupillae muscle, and noradrenaline is neurotransmitter. The sympathetic fibres also contain vasoconstrictors to the facial skin and stimulate facial sweat glands (see Horners syndrome).Catecholamines are substances consisting of catechol (an aromatic structure with two hydroxyl groups) linked to an amine. The synthesis is described in Chapter 29.Catecholamines increase heart rate and cardiac output by stimulation of the adrenergic b1-receptors in the myocardium. Catecholamines, released by the adrenal medulla, support the sympathetic system by modifying the circulation during exercise. During exercise the blood is directed to the working muscles from other parts. Noradrenergic nerve fibres innervate blood vessels all over the body. Sympathetic innervation accounts for vascular tone and vasoconstriction.The most important exercise response in humans is a tremendous vasodilatation in the vascular bed of muscles. The vasodilatation is probably due to a decrease in the a-adrenergic tone of muscular arterioles, and to the action of adrenaline on b2-receptors.Catecholamines dilatate the bronchial airways by stimulating adrenergic b2-receptors. They increase both tidal volume and respiratory frequency. The result is increased ventilation. Catecholamines acting on b1-receptors cause increased cardiac output. Catecholamines relax the smooth muscles of the digestive tract (b2-receptors), but contract the sphincters. Catecholamines stimulate metabolism (by activation of the thyroid hormone, T3) and lipolysis. Adrenaline stimulates hepatic glycogenolysis via b2-receptors.Finally, adrenaline stimulates the ascending reticular system (ie, the reticular activating system or RAS) in the brain stem, thus keeping us alert and causing arousal reactions with desynchronisation of the EEG (Chapter 10).The resistance vessels of the striated muscles in hunting predators (and perhaps in humans) are also innervated by another system. This is the cholinergic, sympathetic vasodilator system. It is capable of a rapid and appropriate bloodflow response during hunting.Acute stress activates the splancnic nerves and liberates large amounts of adrenaline from the medulla. Diabetics who are developing acute hypoglycaemia, secrete large amounts of catecholamines. Acute muscular activity starts a large catecholamine secretion in exercising persons.Besides catecholamines, ACTH is also released during stress by increasing hypothalamic signals. ACTH stimulates the glucocorticoid and to some extent the mineralocorticoid secretion through cAMP. Small amounts of glucocorticoids are permissive for the actions of catecholamines.Plasma catecholamines are rapidly removed from the blood and have a half-life in plasma of less than 20 s. This is the combined result of rapid uptake by tissues and inactivation in the liver and vascular endothelia (see Chapter 29). The Autonomic Control Of The Cardiovascular System The brainstem is the primary site for the autonomic cardiovascular control.High-pressure baroreceptors are distension-activated stretch receptors located in the walls of the carotid sinus and the aortic arch. Increased arterial blood pressure increases the signal frequency in the sensory baroreceptor neurons that project into the medullary cardiovascular centre (ie, the solitary tract nucleus, nucleus ambiguus and the dorsal motor nucleus of the vagus, DMNV). Impulses generated in the baroreceptor neurons with increasing blood pressure, activate the vagal efferents to the heart and inhibit the sympathetic tone towards the heart. As a consequence the heart rates and force of contraction decreases. Impulses generated in cardiac baroreceptors by cardiac filling, also activate the force of contraction (Fig. 6-4).The postganglionic fibres from the 3 upper cervical ganglia of the sympathetic trunk pass to the heart as the cardiac nerves to the cardiac plexus.
Fig. 6-4: The autonomic control of blood pressure and heart rate.The sympathetic effect is dominant. Increased sympathetic activity constricts the veins, which increases cardiac output by augmenting cardiac filling. Arteriolar constriction reduces cardiac output by increasing the arterial blood pressure (ie, afterload). Other sensory inputs from skeletal muscles, lungs, gastrointestinal viscera, hypothalamus and forebrain help to co-ordinate the autonomic cardiovascular responses related to exercise, respiration, and feeding and temperature control. Hormones, such as angiotensin II, can also modulate the autonomic responses through neurons in the circumventricular organs of the brain, These organs (such as the area postrema) lack the blood-brain barrier.The sympathetic system innervates the sinus node, the coronary vessels and the myocardial syncytium. Each fibre ends in many terminals, and from the terminals the transmitter noradrenaline is released to the b2 -receptors of the smooth muscle cells of the coronary vessels and of the myocardium (Fig. 6-4). As a result of increased sympathetic tone, the contractility of the myocardium is increased. Thus, the end systolic volume falls from its usual volume- as an example from 70 ml to 40 ml, and the end diastolic volume increases due to increased venous return of blood from 140 to 180 ml. Hereby, the stroke volume is increased from 70 to 140 ml of blood in the example. A combination of the doubling of stroke volume with a threefold increase in heart rate, results in a 6-fold rise in cardiac output.Sympathetic stimulation depolarizes the sinus node, so that the threshold potential is reached faster than normal. Hereby, the heart rate is increased, and may reach 220 beats/min in young persons. Such a high frequency is due to a maximal sympathetic activation of the heart combined with a reduction of the vagal tone. Activation of noradrenergic fibres leads to peripheral sympathetic vasoconstriction, so that blood is shunted to central areas. The heart is stimulated through b1-receptors so that its frequency and contractility is increased. Other organs are also stimulated to make the person fit for fight or flight in any stressful situation.The postganglionic sympathetic fibres have noradrenaline and ATP containing vacuoles in their nerve terminals. Hence, they release noradrenaline and ATP. The noradrenaline is produced in the chromaffine granules of the neuron.
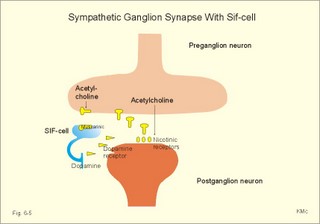
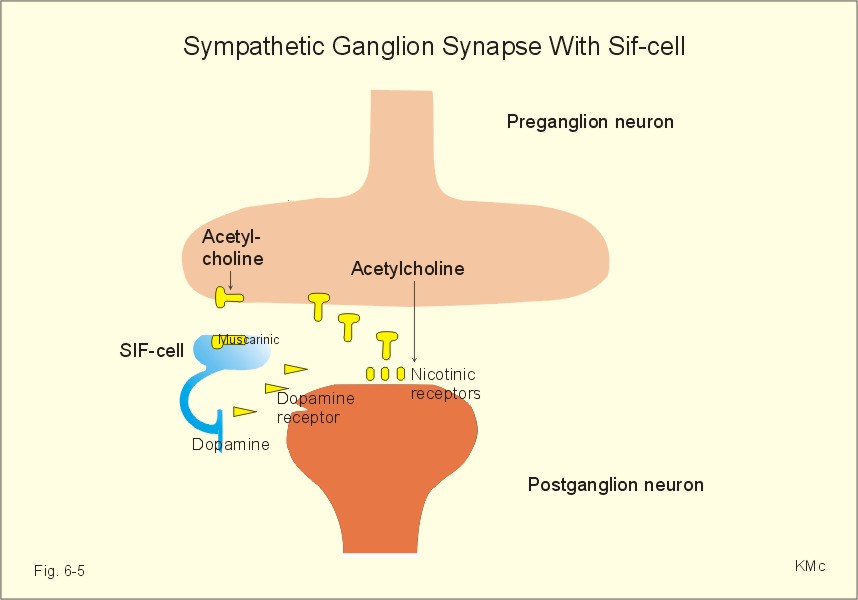
Fig. 6-5: A sympathetic ganglionic synapse with a small intensity fluorescent cell (SIF cell).Acetylcholine is released from the preganglionic cell and binds to nicotinic receptors on the postganglionic cell. Acetylcholine also binds to small SIF cells (Fig. 6-5) with muscarinic receptors and vesicles that contain dopamine. Dopamine interacts with dopamine receptors (D2 and D4) on the postganglionic cell and modulates ganglionic transmission by increased permeability to small ions and hyperpolarisation.Liberation of noradrenaline and ATP to the blood does not only lead to constriction of arterioles and arterial vessels, but also constriction of veins and venules. Without venous constriction, the large venous compliance would cause an inordinate amount of blood to be stored in the veins upon sympathetic arteriolar constriction. The consequence would be decreased venous return, which decreases cardiac output and perfusion of vital organs.Activation of presynaptic purine receptors by adenosine inhibits adrenaline release from the postganglionic terminals innervating the blood vessels. This results in massive vasodilatation.Exercise and stress demand mobilisation of energy to muscles and heart. Activation of b2-receptors in the arteriolar wall by circulating catecholamines from the medulla also contributes to vasodilatation in the striated muscles. The total peripheral vascular resistance is reduced during exercise to 20-30% of resting values.During stress the cutaneous circulation is reduced at first, but then the cutaneous bloodflow rises due to the increased heat production. The brain vessels are only modestly constricted by sympathetic stimulation. The parasympathetic system has two subdivisions. The cranial division in the brainstem innervates the blood vessels of the head and neck and of many Thoraco-abdominal viscera. The sacral division in the sacral cord innervates the smooth muscles of the walls of the viscera and their glands (the large intestine, liver, kidney, spleen, the bladder and the genitals).The parasympathetic system only innervates a small percentage of the resistance vessels. Only arteries in the brain and of the penis, the clitoris, and the labia minora receive parasympathetic innervation. Hence, the parasympathetic system has a minimal effect on the arterial blood pressure.Parasympathetic fibres travelling in the vagus nerve are of utmost importance in affecting the cardiac rate. Vagal fibres innervate the sino-atrial- and the atrio-ventricular-nodes as well as the atrial muscle walls.The parasympathetic system also innervates the tear and the salivary glands, and the muscles within the eye.Excitation of the vagus decreases heart rate and atrial contractile force, increases intestinal motility, contracts the gall bladder and bronchi, and relaxes the sphincters of the gastrointestinal tract. The vagal decrease in heart rate is due to the rhythm shift to special P cells, which have a slow rate of depolarisation. Acetylcholine (ACh) is liberated on the cardiac cell membranes, ACh-activated K+ - channels are opened (via cholinergic receptors and G-regulatory proteins), and K+ leaks out of the cells, thus opposing the pacemaker current. Vagal stimulation slows down the AV-conduction, causing the co-ordination of atrial and ventricular rhythm to be disrupted. Vagal stimulation can lead to death. Thus external massage of the carotid sinus can cause collar death by greatly increasing vagal stimulation.The effect of acetylcholine released in the autonomic ganglia can be simulated by nicotine. Conversely, the effect of acetylcholine released by parasympathetic nerve terminals at the target organs can be simulated by muscarine. These observations suggest the presence of two different types of cholinergic receptors. Cholinergic receptors are activated by ACh and by metacholine (MeCH).
This paragraph deals with 1. Mushroom poisoning, 2. Carbamate and organo-phosphate poisoning, 3. Xerophtalmia and xerostomia, 4. Tachycardia and bradycardia, 5. Smoking, 6. Phaeochromocytoma, 7. Primary or essential hypertension, 8. Horners syndrome, 9. The Kluver- Bucy-syndrome and emotional disorders. - Altzheimers disease and Parkinson’s disease are also related to the autonomic nervous system and described in Chapter 7. 1. Mushroom Poisoning Among the poisonous mushrooms at least two are related to the autonomic nervous system: Amanita palterina (false blusher) contains a substance with atropine-effect, which completely blocks the muscarinic cholinergic receptors. Atropine-effects are described below. Amanita muscaria (red fly agaric) contains atropine-like substances, muscarine and other hallucinogens. Atropine-effects are prominent: Motor unrest, delirium (red fly agaric was used by the Vikings to run berserk), mouth dryness, pupillary dilatation, and tachycardia. Some cases are dominated by muscarine-effects: Glandular secretion (sweat, saliva, tear-flow), miosis, eye pains, bradycardia, cramps, respiratory failure, lung oedema, and coma. Muscarinic symptoms are treated with slow intravenous injection of atropine (1 mg in 1 ml). - Ventilation with the mouth-to mouth-method may become fatal for the rescuer. 2. Carbamate And Organo-Phosphate Poisoning These substances (carbaryle, dimethoate, melathion, parathion etc) are used as insecticides in agriculture. They are anti-cholinesterases so they accumulate acetylcholine in the tissues. The clinical picture is due to the muscarinic and nicotinic effects of acetylcholine. The muscarine-effects are described above. Other symptoms are nausea, vomiting, muscle weakness, paresthesia, bronchospasm, shock and respiratory arrest. Atropine (1 mg iv.) is given repeatedly to obtain complete atropine blockade beginning with pupillary dilatation. Artificial ventilation is often imperative. Cholinesterase- reactivators are tried in desperate situations. 3. Xerophtalmia and xerostomia Xerophtalmia and xerostomia is dryness of the conjunctiva and the cornea, and dryness of the mouth, respectively. Most of these disorders are of unknown origin (ie essential or primary), although an autonomic cause may be suspected. Xerophtalmia and xerostomia occurs in connection with anaesthesia due to the use of atropine-like substances in order to reduce secretion. 4. Tachycardia and bradycardia. A balance between the parasympathetic and the sympathetic system normally determines cardiac rhythm. The parasympathetic system predominates. A relative dominance of the sympathetic tone towards the heart leads to tachycardia (ie, a heart rate above 80 beats per min), and a further relative dominance of the parasympathetic system leads to bradycardia (ie, a heart rate below 50 beats per min). Fluctuations of the autonomic tone leads to phasic changes of the sinus node activity. During inspiration, the parasympathetic dominance falls and the heart rate becomes rapid, whereas during expiration parasympathetic dominance increases and the heart slows down. This phenomenon is found in children, and it can even be found in healthy subjects of high age. The phenomenon is called sinus arrhythmia. 5. Smoking Cigarette smoking is common among teen-agers, and more girls than boys of 15 years smoke cigarettes. Activation of nicotinic cholinergic receptors is fast and does not require G proteins. Nicotinic receptors stimulated by acetylcholine open a Na+-channel and depolarise the cell membrane. Nicotine stimulates nicotinic receptors on the postganglionic neuron of all autonomic ganglia.The number of cigarettes smoked and the number of years smoked seem to increase the number of nicotinic cholinergic receptors in brain tissue. Smoker’s dependency may depend upon the number of nicotinic receptors. Smokers, deprived of the usual daily dose of nicotine in cigarettes, become depressed in mood, they feel stress and they are un-concentrated. This is called abstinence and the cause is lack of nicotine. The mood of the smoker is immediately improved by smoking. Although smoking is nicotine addiction, nicotine seems to be one of the less dangerous molecules in smoke. Polycyclic aromatic hydrocarbons and nitrosamines are potent carcinogens and mutagens. Such substances release proteinases from granulocytes and macrophages, whereby elastin is destroyed resulting in multi-site lung degeneration or emphysema. The life-threatening dangers are due to cancer and atherosclerosis: Lung cancer, chronic bronchitis and emphysema, cerebral stroke, ischaemic heart disease, peripheral vascular disease, bladder cancer, and memory problems. Male smokers have an increase in the number of abnormal spermatozoa, and pregnant female smokers have an increase in neonatal mortality. Female smokers above 30 years using anti-pregnancy pills have a 40-fold higher risk of cerebral stroke than their non-smoking control group. 6. Phaeochromocytoma Some patients suffer from attacks of severe hypertension due to adrenaline hypersecretion. The hypertension is caused by release of large amounts of adrenaline from a medullary tumour of chromaffine cells. The attacks are sometimes fatal. The diagnosis is important, because the patient can be cured by surgical abolition of the tumour. 7. Primary or essential hypertension in general begins as a condition with sympathetic overactivity (see Chapter 9). 8. Horner’s syndrome refers to a condition with miosis, facial vasodilatation and loss of facial sweating and enophtalmus due to damage of the sympathetic nerve supply from the T1-T2-segments to the eye and facial skin. 9. The Kluver- Bucy-syndrome refers to an emotional disorder with bilateral temporal lobe lesions. The temporal cortex, hippocampus and the amygdaloid body are damaged. Mental blindness (visual agnosia) is the inability to recognise objects seen. Besides mental blindness, the syndrome consists of loss of short-term memory, and hypersexual behaviour incompatible with normal social adaptation. The hypersexual behaviour is related to the visual agnosia. I. Each of the following five statements have True/False options:
II. Each of the following five statements have True/False options:
A 19-year-old female is in hospital with a cranial lesion caused by a fall from her horse. The following clinical signs are found: 1) speech troubles and hoarseness, 2) swallowing problems and paresis of the soft palate, 3) rapid heart rate, and 4) dilatation of the stomach with vomiting. Lesion of a certain cranial nerve can explain all symptoms and signs. 1. What is the name of the nerve? 2. What is special about this particular lesion? Try to solve the problems before looking up the answers .
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
.jpg){kind=link}
{kind=link}
{kind=link}
Click here to introduce your comments or contributions